Pre-visit Considerations
Obstetrician–gynecologists and other reproductive health care professionals should understand the barriers that prevent disabled people from accessing reproductive health care. This is critical in identifying inequities and informing patient-centered approaches to services.
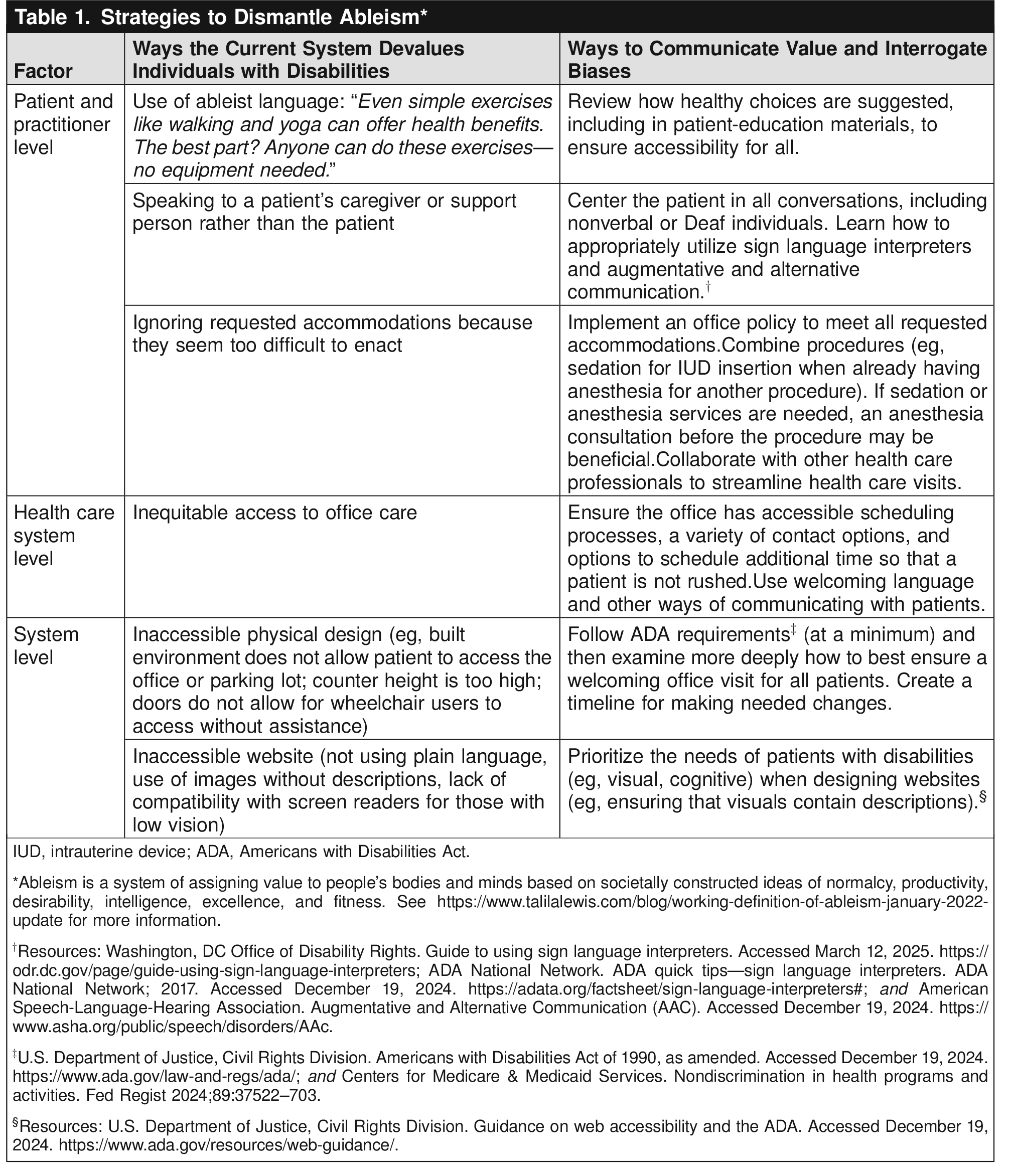
The stated goal of the ADA is, “…to assure equality of opportunity, full participation, independent living, and economic self-sufficiency…” for people with disabilities in the context of “the continuing existence of unfair and unnecessary discrimination and prejudice…” against people with disabilities Box 1 for barriers to care to be identified in a practice.
The Axes of Access
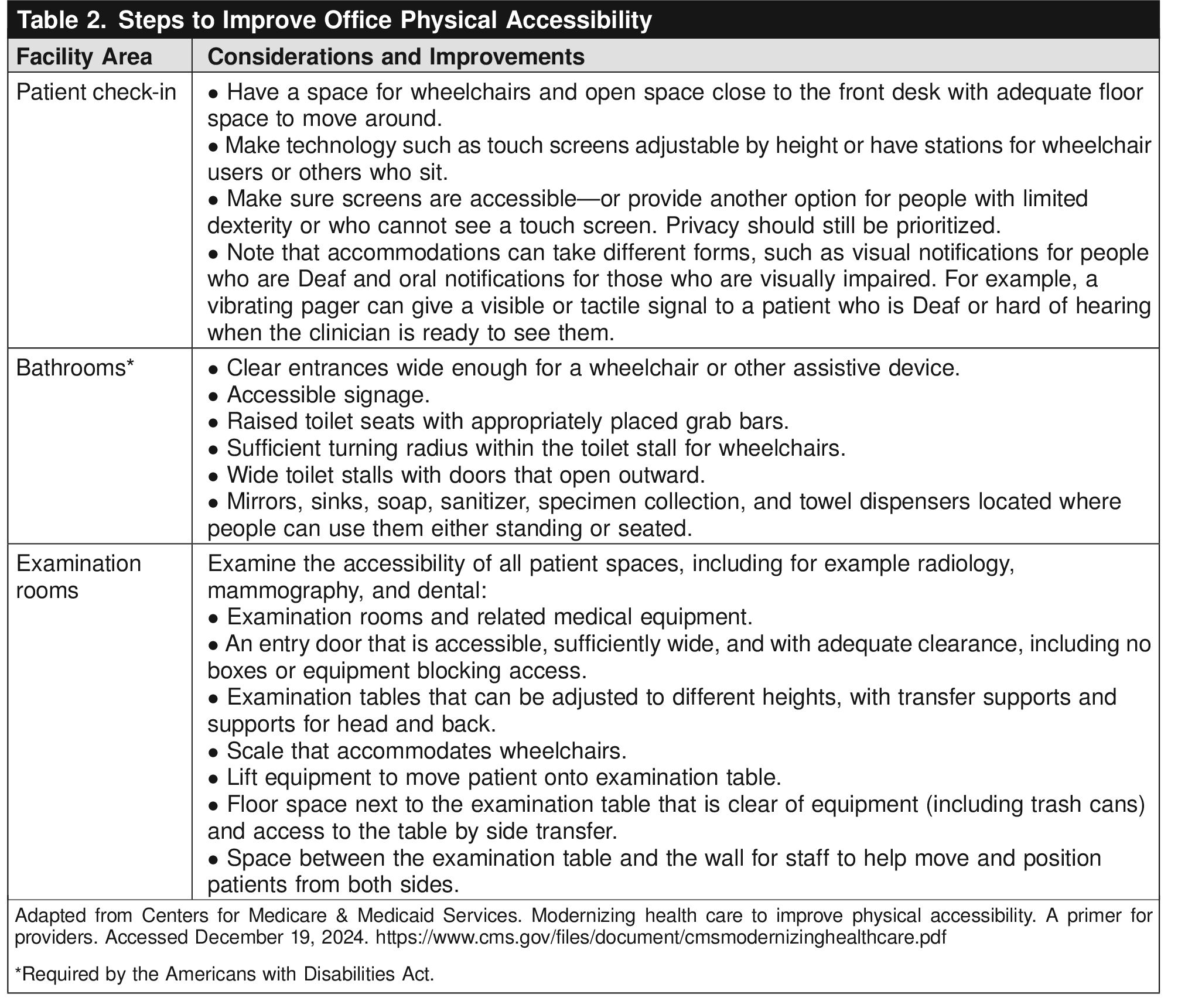
Definition: The health care environment, including care settings, is free of physical barriers to care.
Definition: Policies and procedures promote accessibility of scheduling, staffing, and administrative resources.
Strategies
Policies and procedures should be reviewed and include the following:
Patients are asked about needs for accommodation at the time of the first interaction with a health care provider.
Any special needs are flagged in the scheduling system and electronic record.
When patients are expected for an appointment, accessible equipment and staff are reserved.
Service animals that are qualified under ADA provisions are allowed.
Staff are correctly trained in disability etiquette (eg, a wheelchair is part of the patient's personal space) and methods of transfer.
Communication policies are reviewed.
Communication access
Definition: Provider and system factors do not limit a patient's ability to make an appointment, arrange for follow-up, understand goals of care, or adhere to prescribed therapy.
Strategies
Printed forms are available in large font and in modified versions that accommodate patients who have low literacy.
American Sign Language interpreters are available free of charge.
Amplification devices for patients with impaired hearing are accommodated.
E-mail or text messaging is allowed to make appointments and communicate with providers.
Work is done to change systematic problems (eg, hard-to-read prescription labels).
ADA, the Americans with Disabilities Act.
Reprinted from Lagu T, Iezzoni LI, Lindenauer PK. The axes of access--improving care for patients with disabilities. N Engl J Med 2014;370:1847–51.
doi: 10.1056/NEJMsb1315940. Copyright© 2025 Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society.
The degree of difficulty accessing care varies by patient. Where possible, practices should consider universal design. The intent of universal design is to simplify life for everyone by making products, communications, and the physical environment more usable by as many people as possible at little or no extra cost 16. Universal design benefits people of all ages and abilities, although it does not replace the need for accommodations for all people with disabilities. When required, health care professionals must provide individualized accommodations based on a patient's individual needs. Additionally, ACOG encourages adoption of hiring practices at health care institutions and practices that provide for a diverse staff, including individuals with disabilities.
Screening Considerations
Patients with disabilities should have access to the same health care as all patients, including all age-appropriate screening tests. It is important that health care teams acknowledge their inherent biases and offer and facilitate access to appropriate care, including recommended screening tests.
Breast and Cervical Cancer Screening
Like all patients, individuals with disabilities require preventive services. However, there are consistent disparities in rates of breast and cervical cancer screening for disabled patients when compared with the general population. A 2021 review of National Health Interview Survey data determined that patients with self-reported disabilities, including those with movement difficulties and complex activity limitations, had a higher likelihood of breast and cervical cancer diagnoses compared with the general population 27. Data from the 2020 Behavioral Risk Factor Surveillance System and the 2021 National Health Interview Survey showed that women with any disability were less likely to have received a mammogram in the previous 2 years and less likely to be up to date on cervical cancer screening than women without disabilities Screening for Intimate Partner Violence and Sexual Abuse
Having a disability is a known risk factor for intimate partner violence, and individuals with disabilities are at nearly double the lifetime risk of intimate partner violence victimization as those without disabilities 29. Individuals with physical and developmental disabilities may be reliant on their partners or caregivers for help, creating a dangerous dynamic in which abusers may be in a position to physically abuse their victims by withholding medication, preventing use of assistive equipment such as canes or wheelchairs, and sabotaging other personal service needs such as help with bathing, bathroom functions, or eating 30.
Although disability communities are diverse and abuse is experienced differently, the rate of sexual abuse in patients with disabilities, particularly those who need personal caregivers, is high. A 2021 systematic review and meta-analysis of U.S. and international data showed a 31.3% prevalence rate of unwanted sexual activity in women with intellectual disabilities; the rate of abuse was found to increase as the severity of the intellectual disability increased 31. A 2020 study reported that 25% of women with Down syndrome had experienced unwanted sexual advances 32. Although it can be challenging to screen for sexual abuse in patients who present to care with family members or caregivers, it is essential to incorporate these screening practices into routine care to safely identify patients at risk.
Additionally, women with disabilities are at greater risk of physical abuse during pregnancy. A study of the Massachusetts Pregnancy Risk Assessment Monitoring System data found that women with disabilities were three to four times more likely to experience abuse before and during pregnancy than pregnant women without disabilities 33. Nevertheless, in a qualitative study of U.S women with limitations in hearing, vision, cognition, mobility, self-care, and independent living, eight of the nine respondents (89%) reported that no health care professional had ever asked them about violence during their pregnancies 34.
Screening for Sexually Transmitted Infections
All patients should be screened for STIs and offered testing in accordance with Centers for Disease Control and Prevention guidelines 35. Data suggest that health care professionals who care for patients with physical and intellectual disabilities often assume patients are not sexually active, avoid asking questions about sexual history and activity, and fail to provide sexuality education information. Although data on rates of STIs in patients with intellectual disabilities are lacking, the increased risk of abuse and lack of access to sexuality education for many patients makes screening especially important 36. Oftentimes, individuals might not have the ability or feel safe to disclose abuse, putting patients at risk for unidentified STIs. Clinicians should keep in mind that STIs also may be the result of consensual sexual relationships.
Reproductive Health Care Services
Patients with disabilities should be provided access to the full range of reproductive health services, including comprehensive contraceptive counseling and prenatal and abortion care. This care should be offered in a safe and welcoming manner.
Menstrual Hygiene
Anticipatory guidance before menarche can be very useful and may lessen anxiety felt by patients and caregivers 37. Some patients with difficulty managing menstrual blood loss due to physical disability or intellectual disability may be candidates for hormonal suppression of menses. Other individuals may be seeking education on menstrual health. A 2020 study of young women with Down syndrome demonstrated that, although they were less likely to access reproductive health care compared with the general population, more than half of them received medication for menstrual issues 32. For more details on options for and approaches to menstrual suppression, see ACOG Clinical Consensus No.3,
General Approaches to Medical Management of Menstrual Suppression 37.
Contraceptive Access
Sexuality is a human right, and individuals with disabilities have the same right to sexual expression as their peers without disabilities. Education on reproductive health, expectations for fertility, and discussions about healthy relationships are important for all patients, and ob-gyns should engage their patients with disabilities in these discussions. As noted by the National Partnership for Women and Families, the ability to control one's own reproductive life allows individuals with disabilities to participate fully in society 39, even if this conflicts with the wishes of their caregivers. This may require helping patients to navigate getting care without their trusted caregiver for the first time or helping to navigate challenging conversations with the patient and caregiver. With access to and support for sexual expression, many of these patients will require access to contraceptive choice. The American College of Obstetricians and Gynecologists recommends the use of a patient-centered reproductive justice framework and a shared decision-making model in the provision of supportive contraceptive counseling and care to help patients achieve their reproductive goals 40.
There is a long history of forced sterilization of patients with disabilities, resulting in the erosion of trust in the health care system. See ACOG Committee Statement No. 8,
Permanent Contraception: Ethical Issues and Considerations, for further details on counseling considerations for permanent contraception 41. Patients require full access to information about various contraceptive methods, including adverse effects. As with all patients who seek reproductive health care, ob-gyns should engage individuals with disabilities in patient-centered contraceptive counseling and offer the full spectrum of contraceptive care, from initiation to discontinuation.
Abortion Access
The changes in the national legal landscape of abortion access will further marginalize individuals with disabilities 43. It is critical that health care professionals who provide reproductive health care continue to advocate for equitable access to care for all patients and guard against potential reproductive coercion from partners or caregivers 44.
Pregnancy and Parenting
A 2018 study of National Survey of Family Growth data found that 19.5% of birthing respondents had at least one disability, which is similar to the prevalence of disability among all women of reproductive age in the United States 45. A 2017 study demonstrated that women with disabilities are as likely as their nondisabled peers to desire pregnancy (61% and 60%, respectively), but fewer intend to have a baby in the future (43% and 50%, respectively) 46. More research is needed to further identify factors that affect the desire of an individual with a disability to parent and barriers that could be eliminated.
In addition to negative attitudes from the general public toward the parenting abilities of individuals with disabilities, studies widely document that patients with disabilities have had negative experiences with obstetric care professionals who may doubt a patient's ability to parent, carry a pregnancy, and deliver safely 46. This bias contributes to delays in accessing prenatal care or avoiding it altogether. A 2022 study of National Survey of Family Growth data found that, in comparison with those without disabilities, women with disabilities were more likely to have smoked during pregnancy, delayed entry into prenatal care, given birth prematurely, and have had a neonate with low birth weight 47. Other studies have shown similar increased associations with adverse conditions in the pregnancies of individuals with disabilities, including gestational diabetes, hypertensive disorders, and increased risk of cesarean delivery 48. According to experts, given the risk factors women with disabilities have going into pregnancy, there likely is an increased theoretical risk of maternal mortality 49. All-cause mortality among community-dwelling adults with any disability is increased compared with adults without disabilities (adjusted hazard ratio 1.51, 95% CI, 1.45–1.57), with a greater magnitude of the association between disability and death in young and middle-aged adults (age 18–64 years) 50. Patients should receive evidence-based counseling about their individual risks in pregnancy based on specific medical conditions, avoiding making generalized assumptions about limitations that may be associated with disability. Genetic screening should be discussed and offered according to typical office guidelines for all patients, but consideration should be given that there is a perception of inherent ableism built into genetic screening that can be offensive to some patients.