Number 11 (Replaces Committee Opinion Number 729, January 2018)
This Committee Statement was developed by the American College of Obstetricians and Gynecologists’ Committee on Advancing Equity in Obstetric and Gynecologic Health Care in collaboration with Beth Cronin, MD, Michelle Moniz, MD, MSc, and Noah Nattell, MD, MS.
ABSTRACT: Social and structural determinants of health include historical, social, political, and economic forces, many of which are rooted in racism and inequality, that shape the relationship between environmental conditions and individual health. Unmet social needs can increase the risk of many conditions treated by obstetrician–gynecologists (ob-gyns), including, but not limited to, preterm birth, unintended pregnancy, infertility, cervical cancer, breast cancer, and maternal mortality. An individual health care professional’s biases (whether overt or unconscious) affect delivery of care and may exacerbate and reinforce health disparities through inequitable treatment. Obstetrician–gynecologists and other health care professionals should seek to understand patients’ health care decision making not simply as patients’ individual-level behavior, but rather as the result of intersecting sociopolitical conditions, structural inequities, and social needs that create and maintain inequalities in health and health care. Recognizing the importance of social and structural determinants of health can help ob-gyns and other health care professionals to better understand patients, effectively communicate about health-related conditions and behavior, and contribute to improved health outcomes, including patients’ experience of care and their trust in the health care system.
Summary of Recommendations and Conclusions
Based on the principles outlined in this Committee Statement, the American College of Obstetricians and Gynecologists (ACOG) makes the following recommendations and conclusions:
Health care professionals should be aware of and understand the social and structural drivers that affect health outcomes. They should acknowledge that race, institutionalized racism, and other forms of discrimination serve as social determinants of health.
To provide patient-centered care, each routine office visit should include appropriate questions about social and structural drivers of health that may influence a patient’s health and use of the health care system. It is important to be cognizant that screening for social and structural drivers may not elicit open responses from all patients due to perceived stigma or fear of negative consequences (eg, social services involvement) or both.
An individual health care professional's biases (whether overt or unconscious) affect delivery of care and may exacerbate and reinforce health disparities through inequitable treatment.
Obstetrician–gynecologist practices that are part of a community health care clinic or larger networks should encourage their facilities to establish medical–legal partnerships.
Health care professionals should maximize referrals to appropriate services to help improve patients’ abilities to fulfill needs identified by screening for social and structural determinants of health.
Health care professionals should be aware of and make allowances for transportation and other logistical difficulties and differences.
Health care professionals should advocate for policy changes that promote safe and healthy living environments.
Background
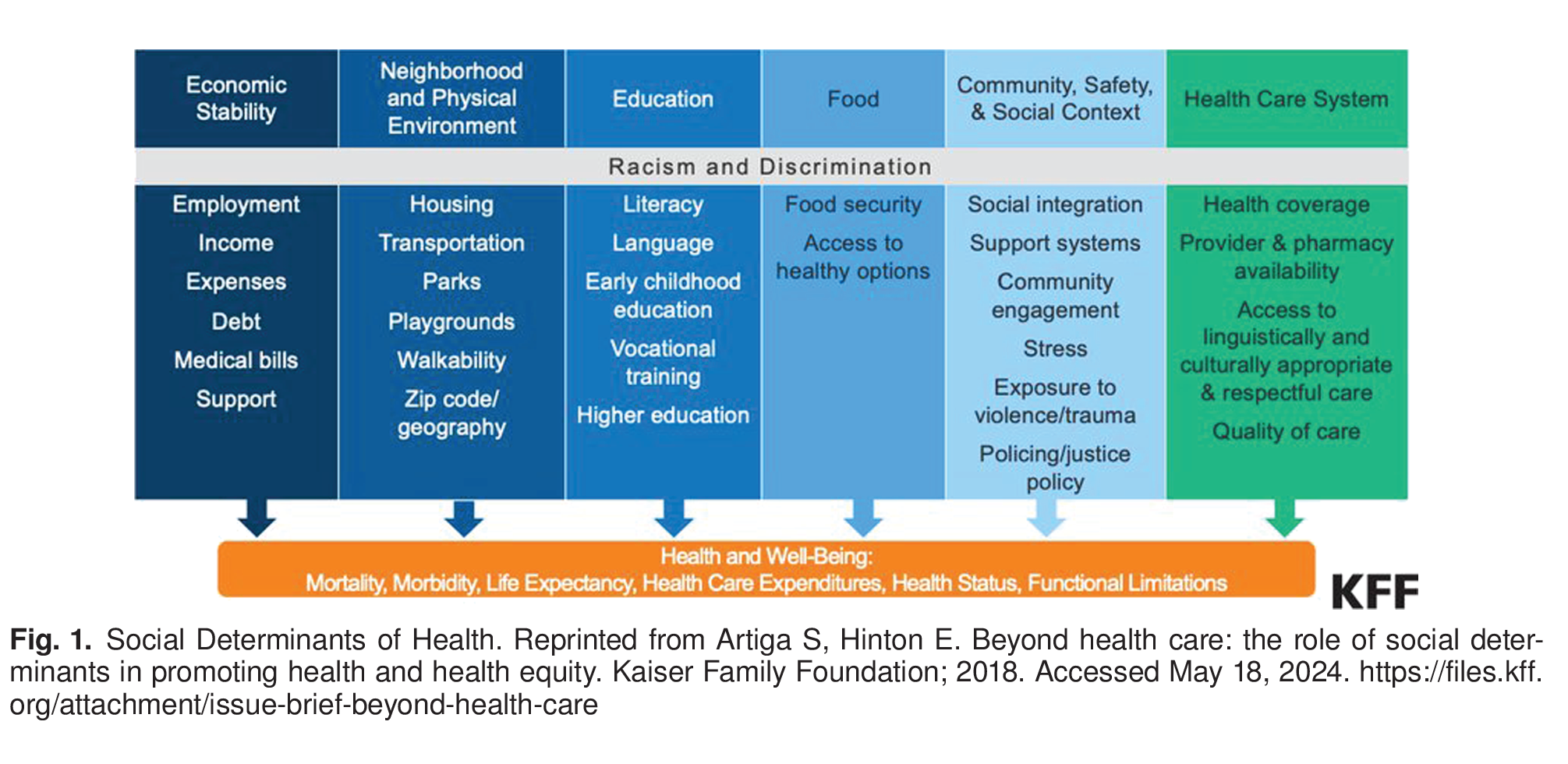
Social determinants of health are the conditions in which a person is born and lives that affect their health; this includes access to safe housing, adequate food, and clean water. Structural determinants of health are the macro-level effects, such as the economic, social, and political systems that influence and drive disparities in health outcomes 2. Social and structural determinants (often abbreviated to “social determinants of health”) include historical, social, political, and economic forces, many of which are rooted in racism and inequality, that shape the relationship between environmental conditions and individual health 5 6 7 9 Figure 1. Environmental factors account for more than one-third of the total deaths in the United States in a year, and evidence suggests that addressing the social needs of individuals results in improved overall health 10 11 12.

It is well established that social determinants of health are responsible for a large proportion of health inequities that exist in the United States. Structural inequities are the totality of ways in which societies foster discrimination through laws and policies in housing, education, employment, health care, criminal justice, and other social sectors. Structural racism and other structural inequities lead to inequitable distribution of resources, with clear consequences for access to health care and health outcomes. Physical conditions, such as lack of access to safe housing, clean drinking water, nutritious food, and safe neighborhoods, contribute to poor health. Sociopolitical conditions, such as the following, all shape the psychological and biological processes that ultimately influence individuals' health and the health of communities: structural racism; police violence targeting Black and Brown individuals; gender inequity; discrimination against lesbian, gay, bisexual, transgender, queer+ (LGBTQ+) individuals; poverty; lack of access to quality education and jobs that pay a livable wage; and mass incarceration 9 13 15 16. Such social conditions not only influence individual health but also work to create cycles that perpetuate intergenerational disadvantage.
Unmet social needs can increase the risk of many conditions treated by obstetrician-gynecologists, including, but not limited to, preterm birth, unintended pregnancy, infertility, cervical cancer, breast cancer, and maternal mortality 17. The social determinants of health approach also acknowledges intersectionality, a term first coined in 1989 by legal scholar Kimberlé Crenshaw, which describes the overlapping categories of social identities, such as gender, race, class, disability status, sexual orientation, and related structures of oppression and discrimination, as they manifest in health care and outcomes. The reproductive justice framework, first developed in 1994 by the Women of African Descent for Reproductive Justice 19. A shared history of discrimination among Black patients negatively influences health outcomes due to mistrust of health care systems 20. This also may be true for LGBTQ+ patients seeking sexual and reproductive health care 21. The intersection between individuals with disabilities and social determinants of health is complex—socioeconomic status, exclusion from education and employment, and poor living conditions add to the risk of poor health outcomes for those with disabilities 23 24. In addition to the mistrust of the health care system, historical racist practices in medical care have contributed to negative outcomes. Continual work needs to be done to eliminate implicit biases and to examine the role that racism plays in ongoing inequitable outcomes.
Examples of Social and Structural Determinants of Health
Awareness of the broader historical and contemporary social contexts that influence health supports respectful, patient-centered care that incorporates lived experiences, optimizes health outcomes, improves communication, and can help reduce health and health care inequities. For example, a pregnant patient with gestational diabetes who has not checked her blood sugar may be labeled as irresponsible or nonadherent. An approach that recognizes the effects of social determinants of health may probe deeper and discover that the patient lacks stable housing and forgets to bring her glucometer each time she moves to another family member's or friend's house. Communicating with this patient about the importance of blood sugar monitoring as the only strategy to address glycemic control would be ineffective. Rather, linking to services to address her housing issues would be much more likely to enable her to manage her gestational diabetes. Another example is a pregnant patient with poor weight gain who is evaluated for medical comorbidities, when deeper questioning into the etiology reveals she was fired from her job and cannot afford enough food for herself and her two children. Ordering tests or discussing the importance of good nutrition in pregnancy would be meaningless if not accompanied by referrals for food assistance. Another commonly encountered scenario influenced by social determinants of health is the ability of patients to arrive at scheduled appointments on time. Many patients with low incomes rely on often unpredictable public transportation and may arrive late to appointments and be forced to reschedule, which creates the impression of nonadherence. Such examples highlight the importance of inquiry into the underlying reasons for these care challenges. In fact, asking about certain social factors can be timesaving in some circumstances, because they can help to address systemic barriers to health care. This strategy has been shown to reduce health care professional burnout and decrease health disparities and also may reduce health care spending 25.
Screening, Social Interventions, and Referrals
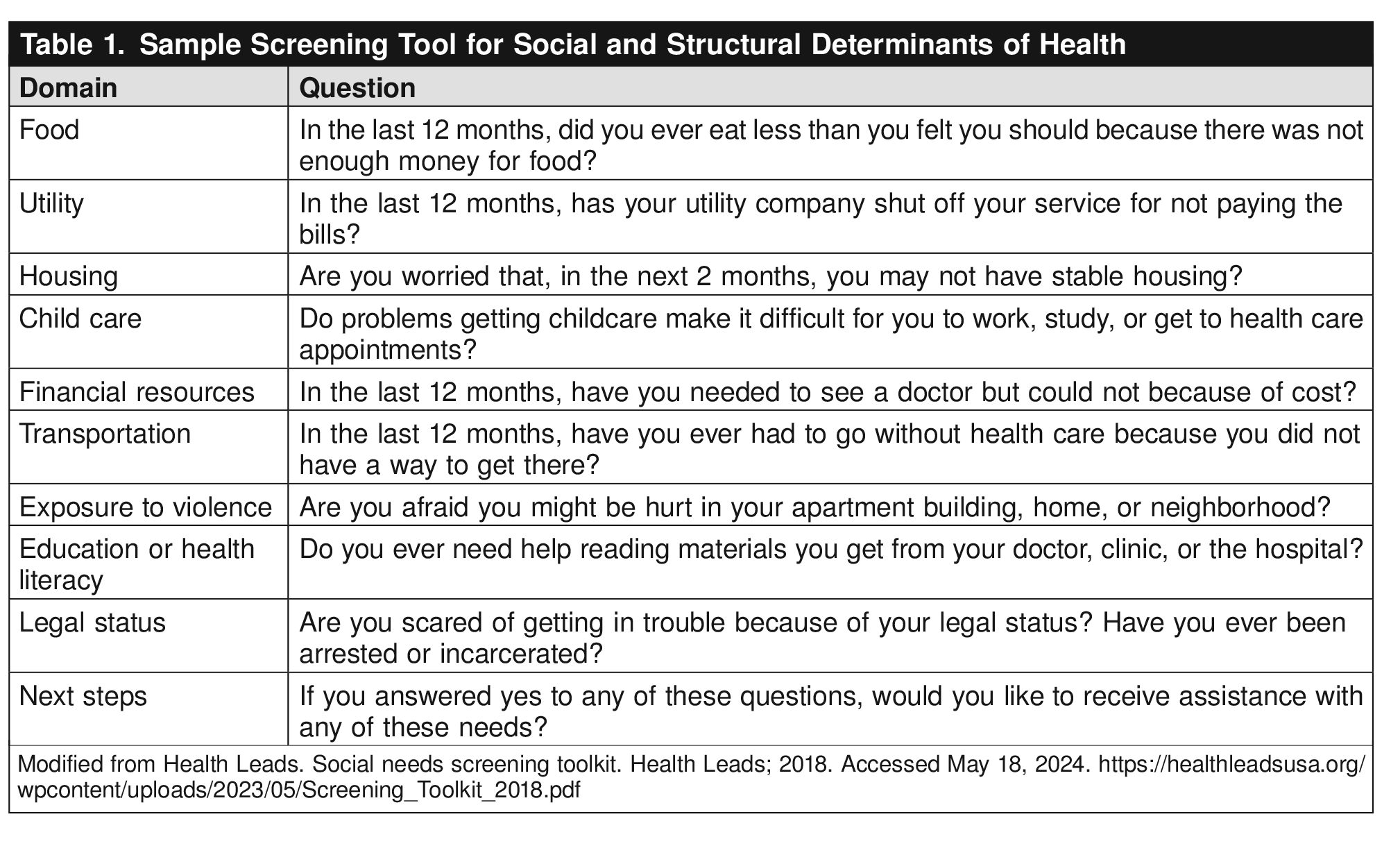
Most physicians recognize the important role social determinants play in health outcomes. In one survey, 85% of physicians felt that patients’ social needs were as important to address as their medical needs, yet 80% felt they were not confident in addressing them 25 27. Including social-indicator prompts in physician-encounter tools has been shown to increase referrals to social services 25. See Table 1 for examples of screening questions for social determinants of health.

Providing referrals to housing or food services while patients are in the clinic can improve their health care usage 25. It is critical that health care professionals use evidence-based, patient-centered approaches to address unmet social needs; many patients referred to social interventions never use them due to factors such as fear of discrimination, cost concerns, and lack of availability during times that work for their family schedule 28. Patients are more likely to engage with social interventions if they believe they will benefit them, the referral is presented in an acceptable way that matches their preferences, the activity is accessible, and transportation to the first session is supported, if needed 28. The provision of interventions to address unmet social needs has been described in an approach called “structural competency” 9. This framework recognizes that the way society is structured (for example, through racial, economic, and gender inequalities) influences clinical interactions and health outcomes. Structural competency aims to help health care professionals intervene on these upstream contributions to disparate health outcomes and to recognize that these structural explanations have limitations and are not comprehensive 9.
Cultural Awareness, Humility, and Sensitivity: Approaches to Care
In the 1990s, a concerted recognition emerged among health care professionals and educators that patients come from diverse cultural backgrounds that may influence their understanding of health and illness, interactions with health care professionals and institutions, and engagement with treatment recommendations 29. This was formalized into the framework of “cultural competence,” which provided health care professionals with tools to address cultural differences in their patient care interactions. It aims, in part, to understand patients' health-related behaviors as resulting from their cultural beliefs, beliefs that may influence patients' health care decision making. Title VI of the Civil Rights Act of 1964 requires recipients of federal financial assistance to take reasonable steps to make their programs, services, and activities accessible by eligible persons with limited English proficiency 31. Categorizations such as race and class often are reduced to cultural positions rather than complex political, social, historical, and economic phenomena. Moreover, cultural competency overlooks the cultural dimensions of health care systems and health care professionals themselves. The emphasis on cultural beliefs tends to simplify patients' behavior into basic individual choices, which impedes a deeper understanding of complex interactions of the social, economic, political, and environmental circumstances of patients' lives.
Despite the limitations of a cultural competency approach, it is nonetheless critical for health care professionals to recognize that both patients and health care professionals hold their own set of values stemming from individual life experience and, in some cases, cultural backgrounds. It may be especially helpful, for instance, for a health care professional working in a locale with a large population of immigrants from a particular country to learn about cultural specificities of that group, recognize variations within that group, and understand the overlaying general experience of being an immigrant.
Instead of “competence,” which mistakenly implies that culture is a skill that one can master, other ways to recognize that culture matters in certain clinical encounters include cultural humility, cultural awareness, cross-cultural care, and cultural respect 32 33 35.
Use of Language
The American College of Obstetricians and Gynecologists recognizes and supports the gender diversity of all patients who seek obstetric and gynecologic care. In original portions of this document, authors seek to use gender-inclusive language or gender-neutral language. When describing research findings, this document uses gender terminology reported by investigators. To review ACOG’s policy on inclusive language, see https://www.acog.org/clinical-information/policy-and-position-statements/statements-of-policy/2022/inclusive-language.
Recommendations and Conclusions
Health care professionals should be aware of and understand the social and structural drivers that affect health outcomes. They should acknowledge that race, institutionalized racism, and other forms of discrimination serve as social determinants of health.
It is essential that ob-gyns be aware of the factors that may promote inequity in the clinic and hospital setting. To dismantle racist and discriminatory policies and practices, there must be an understanding of the historical context, as well as how such biases permeate contemporary medicine. Acknowledgement of one's individual implicit and explicit biases is important to best understand the true effects that social and structural determinants of health have on an individual’s choices. That is, it is not simply “noncompliance” when a patient does not follow recommended clinical advice. Review of protocols and implementation of new policies should be scrutinized to ensure equitable access and outcomes and to reduce discriminatory practices. Certain practices, such as urine toxicology screening or referral to child protective services for clinical nonadherence, may be implemented with unintended racial bias but may result in substantial harm for Black and Brown patients.
To provide patient-centered care, each routine office visit should include appropriate questions about social and structural drivers of health that may influence a patient's health and use of the health care system. It is important to be cognizant that screening for social and structural drivers may not elicit open responses from all patients due to perceived stigma or fear of negative consequences (eg, social services involvement) or both.
Social and structural drivers of health should be included in patient-completed intake questionnaires and expanded medical history questions and integrated into electronic medical records prompts. At each routine office visit (eg, prenatal care, well-person visits, preoperative evaluations), health care professionals should inquire about and document social and structural determinants of health that may influence a patient’s health and use of health care, such as access to stable housing, food, and safe drinking water, as well as utility needs, safety in the home and community, immigration status, employment conditions, social integration and support, and freedom from discrimination. Before initiating these screening questions, health care professionals should counsel patients that these data are being collected to help identify necessary services and that they will not be reported or used in ways that could harm them or their families. Patients should be aware of mandatory reporting requirements before investigating such factors. Patients may be hesitant to give honest answers due to the fear of incarceration or involvement of the judicial system, depending on answers given. Health care professionals should be aware that questioning regarding social and structural determinants and social service referrals can be stigmatizing; a patient–doctor relationship of respect and trust is needed to ensure that patients feel safe. When purchasing or customizing electronic medical records for the office, ob-gyns and other health care professionals should request structured fields that capture information on social and behavioral determinants 15 27 36 9 38. Individual ob-gyn practices may not be able to have such services on location, but relationships can be developed with existing medical–legal partnerships to provide necessary services. Obstetrician–gynecologists should advocate for support navigators and care managers who can liaise with health care professionals to address needs identified by screening for social determinants. Larger health care systems, hospitals, and state agencies should work to provide support for legislative policy change to improve resources to address social and structural determinants of health.
Health care professionals should maximize referrals to appropriate services to help improve patients' abilities to fulfill needs identified by screening for social and structural determinants of health.
Obstetrician–gynecologists and other health care professionals should develop partnerships with social workers and local community advocates who provide assistance with basic resources such as food pantries and home utility bills. Patients in need may feel less inhibited from using assistance programs when the ob-gyn frames the referral letter to the community assistance program as a prescription, for example, to promote a healthy pregnancy. For more details on methods linking physicians to community social services, see the Health Leads website at www.healthleadsusa.org.
Health care professionals should be aware of and make allowances for transportation and other logistical difficulties and differences.
Historically and intentionally excluded populations often have difficulties obtaining transportation to health care facilities. Therefore, access to public transportation should be considered when planning office locations. Obstetrician–gynecologists should, whenever possible, accommodate patients who may arrive late due to unpredictable public transportation. In addition, patients from disinvested communities often must bring family members to an office visit. To facilitate attendance at health care appointments, ob-gyns and other health care professionals should avoid making arbitrary rules that prevent children and other family members from attending office visits.
Health care professionals should advocate for policy changes that promote safe and healthy living environments.
Obstetrician–gynecologists should promote hospital and clinical policies that combat discriminatory practices. Advocacy also can be external, including working with professional organizations such as ACOG, advocacy groups, and governmental bodies to identify inequities and enact change. Legislation and governmental policies, including those that address mass incarceration, immigration, housing, and access to reproductive health care, including abortion, have the potential to combat or exacerbate disparities. Obstetrician–gynecologists should use their collective and individual voices to promote patient well-being.
Conclusion
Social and structural determinants of health affect health outcomes as much as biological and individual-level factors. Although cultural competency is advocated to improve patient–health care professional communication, with the ultimate goal of reducing racial and ethnic inequities in health outcomes, the model has significant limitations. Obstetrician–gynecologists and other health care professionals should be aware of these limitations and, rather than solely explain health inequities by cultural differences, recognize that inequities are largely the result of forces that influence health at a point upstream from individual behavior. By understanding these inequities as manifestations of larger social pathologies, health care professionals may begin to address patient needs in a deeper and more effective way. Obstetrician–gynecologists and other health care professionals may address social determinants of health by implementing key practices such as employing multilingual staff, ensuring adequate interpreter services, partnering with medical–legal organizations, and engaging with community resources. These small steps can have an important effect on health outcomes at the individual level and can help reduce health inequities at a population level, resulting in an improvement in patient experiences.
Conflict of Interest Statement
All ACOG committee members and authors have submitted a conflict of interest disclosure statement related to this published product. Any potential conflicts have been considered and managed in accordance with ACOG’s Conflict of Interest Disclosure Policy. The ACOG policies can be found on acog.org. For products jointly developed with other organizations, conflict of interest disclosures by representatives of the other organizations are addressed by those organizations. The American College of Obstetricians and Gynecologists has neither solicited nor accepted any commercial involvement in the development of the content of this published product.