Number 25 (Replaces Committee Statement No. 4, February 2023)
This Committee Statement was developed by the American College of Obstetricians & Gynecologists' Committee on Advancing Equity in Obstetric and Gynecologic Health Care in collaboration with Rose L. Molina, MD, MPH, and Yvonne Butler Tobah, MD.
ABSTRACT: Immigrants face challenges in navigating complex policies that govern access to health care, shelter, food, and clean water, resulting in profound effects on health care outcomes, including increased risk of preterm births and decreased access to preventive health services. These disparities are further exacerbated when immigration policies result in mass detention, incarceration, and deportation, leading to profound trauma among undocumented immigrants and their communities. Obstetrician–gynecologists and other reproductive health care professionals should be prepared to practice immigration-informed care and ensure clinical spaces are welcoming to immigrants. Unless mandated by law, health care professionals should document only information related to a patient's migration history that is necessary for the ongoing clinical care. Health care institutions should provide robust guidance and support for health care personnel and patients faced with the continued complexities of the dynamic landscape of immigration policies. Obstetrician–gynecologists should advocate for the unique needs of patients who are immigrants to promote reproductive justice and health equity.
Summary of Recommendations and Conclusions
Based on the evidence outlined in this Committee Statement, the American College of Obstetricians & Gynecologists (ACOG) makes the following recommendations and conclusions:
Clinicians should know that immigration status is a structural determinant of health that affects access to health care and trust in the health system.
Quality health care should be available for all, regardless of immigration status and ability to pay.
Immigration policies and enforcement practices that lead to family separation and target pregnancy status should be opposed.
People detained in immigration custody settings should be protected from abuse and coercion and should receive obstetric and gynecologic care that complies with accepted evidence-based clinical guidelines and protocols.
The right to seek asylum in the United States should be upheld, including cases related to gender-based violence.
The American College of Obstetricians & Gynecologists opposes policies that allow immigration-enforcement activities or require disclosure or documentation of immigration status within health care facilities.
The American College of Obstetricians & Gynecologists encourages hospitals and other health care institutions to proactively develop policies on interactions with federal immigration and other law enforcement officials to guide clinicians and staff.
Obstetrician–gynecologists are strongly encouraged to work with systems and health care leaders to implement practices to create and protect care settings that are welcoming to immigrants and culturally and linguistically inclusive for all patients.
Obstetrician–gynecologists should promote and support research that monitors the effects of restrictive immigration policies on health care access, utilization, quality, patient experiences, and outcomes.
The American College of Obstetricians & Gynecologists recommends that obstetrician–gynecologists take an active role in local, state, regional, and national advocacy efforts to improve health care access and quality, regardless of immigration status.
Background
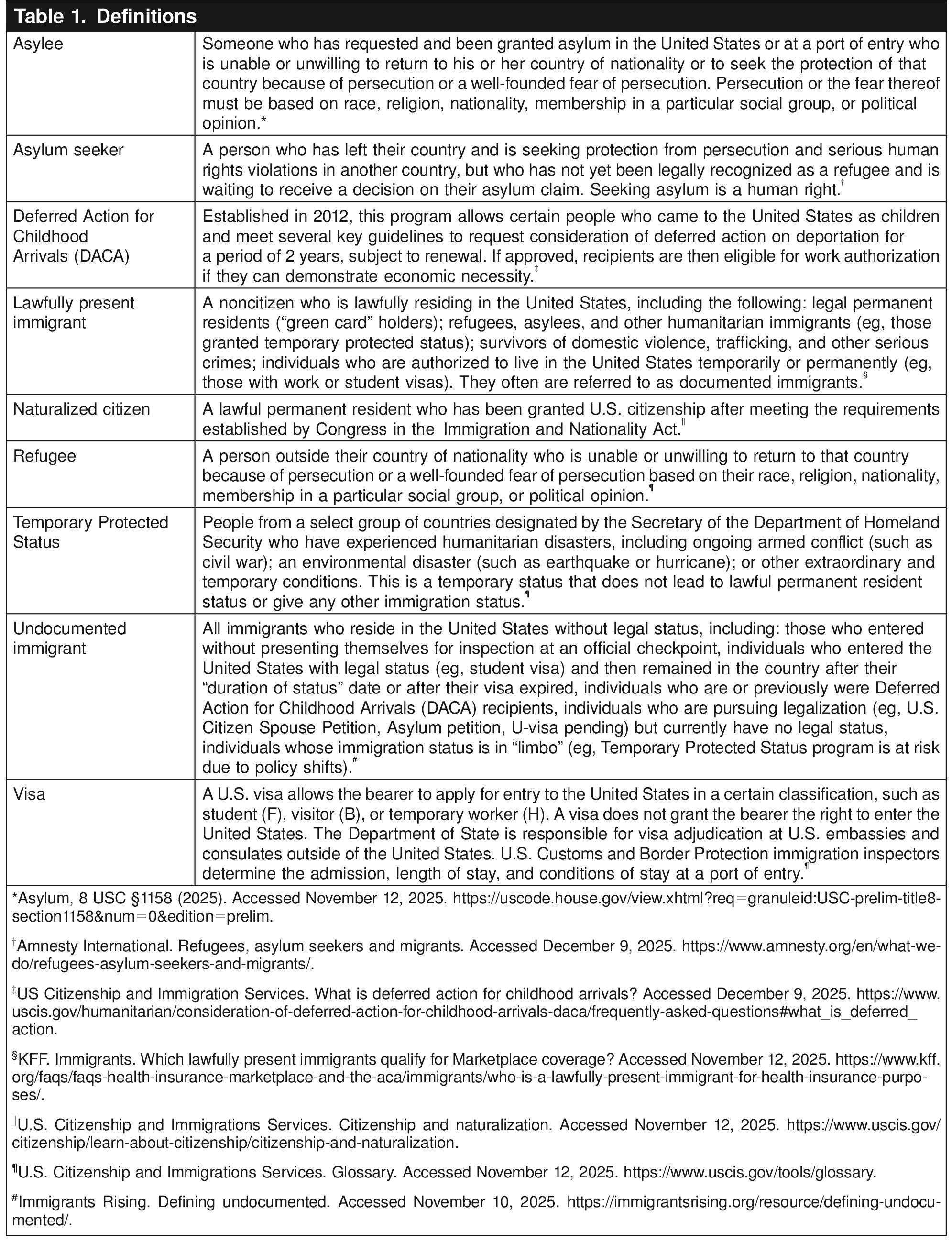
The frequently changing immigration policy landscape makes it difficult to keep statistics about immigration trends and information about eligibility for services updated and easily accessible. This bureaucratic chaos also generates mistrust and fear, because immigration status, which may change over time, confers specific limitations on access to health care and other social services 1. Table 1 summarizes key definitions of common immigration-related terms.

Although the exact number of people in the United States who are undocumented is unknown, the U.S. Department of Homeland Security has reported an estimate of 11 million people who are undocumented 3. Xenophobic public narratives blame undocumented immigrants for using resources; however, many are essential workers in key industries, including agriculture, hospitality, and caregiving, in addition to being valued members of families and communities 4. Increasingly visible and virulent anti-immigrant rhetoric has detrimental effects on the health of individuals, families, and communities 5. In affected communities, studies have shown increases in preterm births and worsening rates of mood disorders, including anxiety and depression 6 7 8 9. Additionally, undocumented immigrants often experience language barriers, fear of seeking services, and anti-immigrant sentiments from clinicians and staff that hinder health care utilization 10. Obstetrician–gynecologists should advocate in solidarity with others against systems and policies that perpetuate racism and xenophobia to improve health outcomes for all 13. Immigration policies that limit access to obstetric and gynecologic care for people in detention, target pregnant people for immigrant-enforcement actions, separate parents and children, and restrict access to asylum for survivors of gender-based violence are in direct conflict with reproductive justice 14. Centuries of discriminatory immigration laws and enforcement activities have sanctioned the dehumanization and cruel treatment of immigrants, with the majority being people of color Clinicians should know that immigration status is a structural determinant of health that affects access to health care and trust in the health system.Recommendations and Conclusions
Structural determinants of health reflect the economic, social, and political systems, which are rooted in racism and social stratification, that shape the relationship between macro-level societal context and individual health 17. Immigration status is a crucial structural determinant of health 18. In addition to the physical and psychosocial risks associated with migration, many newcomers seek refuge from civil or political unrest, poverty, and sexual violence 19. Furthermore, immigrants face challenges in navigating complex policies that govern access to health care, shelter, food, and clean water, resulting in profound effects on maternal and childbirth outcomes, including increased risk of preterm birth 8; decreased access to preventive health services, including immunization 20; and increased risk of maternal morbidity when additional restrictive abortion policies are implemented 21. These disparities are further exacerbated when immigration policies result in mass detention, incarceration, and deportation, leading to profound trauma among undocumented immigrants and their communities. The resulting effects on mental health are associated with increased odds of a lifetime mental health diagnosis among individuals who experience abuse during migrant detention 22. Punitive immigration policies create hostile environments that foster stigma and increase discrimination, stress, and fear of deportation, resulting in heightened anxiety and depression. Such adverse mental health outcomes may also exacerbate preexisting conditions such as high blood pressure, diabetes, and high body fat 24 25. These same barriers limit immigrants' access to contraception and other reproductive health services 26. Although Title X clinics and federally qualified health centers historically have been an accessible source of health care for immigrant communities, they are increasingly under threat, further limiting peoples' access to care.
Undocumented immigrants face unique barriers in accessing gynecologic and obstetric care. Of the types of care that are available to undocumented immigrants, pregnancy care is the most common; though only some states provide prenatal and postpartum coverage 27, and even fewer provide coverage for abortion care 28. Variation in states' pregnancy care coverage leads to a patchwork safety net and inequitable access and outcomes 29. Even with high rates of employment, undocumented immigrants are less likely than U.S. citizens to have health insurance due to reduced access to employer-sponsored coverage and eligibility restrictions that prohibit or delay participation in government-sponsored programs and the Affordable Care Act (ACA) Marketplaces 30 33. If an applicant is deemed likely to require support, that application can be denied.
Restrictive immigration policies lead to cascading effects for both undocumented and documented immigrants, reducing Medicaid participation among eligible immigrants and their families, including U.S.-born children. Many individuals who are undocumented may avoid preventive care completely due to concerns of being targeted, shifting their health care utilization from preventive care to higher-cost emergency services. There are byzantine rules regarding who can access public programs, including prolonged periods before documented immigrants can access them 40. Policies targeting immigrants, including attempts to prevent pregnant people from immigrating and to revoke birthright citizenship, are part of a long history of stratified social hierarchies in which pregnancy, reproduction, and parenting for some individuals is differentially valued compared with others 14.
People detained in immigration custody settings should be protected from abuse and coercion and should receive obstetric and gynecologic care that complies with accepted evidence-based clinical guidelines and protocols.
Consistent with its long history of mass incarceration of marginalized people, starting with the legacy of slavery, the United States has the largest immigration-detention system in the world, with billions of dollars being spent on hundreds of detention facilities overseen by government agencies and private, for-profit companies 41 42. Human Rights Watch has documented physical assault, dehumanizing language, withholding of food as a tool of coercion, and sexual abuse in U.S. detention centers 41. Detainees, especially pregnant people, have poor access to medical care and may have worse health outcomes as a result 42 46. The American College of Obstetricians & Gynecologists supports proposed legislation to ban the shackling of pregnant people in ICE and U.S. Customs and Border Protection custody 19. People with a history of trauma are particularly negatively affected by detention and experience more severe symptoms of anxiety and depression after a period of detention 48; the lack of mental health services in detention compounds this trauma 46 46.
The right to seek asylum in the United States should be upheld, including cases related to gender-based violence.
Seeking asylum is a fundamental human right. International and U.S. law allow for humanitarian protection for people who have been persecuted or fear persecution based on race, religion, nationality, political opinion, or membership in a particular social group 20 52.
Clinicians can support immigrants by performing forensic medical evaluations of people seeking asylum; documenting evidence of torture and ill-treatment is well within the scope of obstetric and gynecologic care. Information about online training for forensic medical evaluations is available at https://asylummedtraining.org/ . Obstetrician–gynecologists should work with their institutions to identify potential barriers and solutions to participating in forensic medical evaluations.
The American College of Obstetricians & Gynecologists opposes policies that allow immigration-enforcement activities or require disclosure or documentation of immigration status within health care facilities.
Institutions such as health care facilities, schools, and places of worship were previously considered “sensitive locations” in which ICE agents refrained from immigration-enforcement activities. This policy was rescinded in 2025, allowing ICE agents to seek information and forcefully detain individuals in these settings 54. Such immigration-enforcement activities also may negatively affect the health care workforce and other patients by provoking anxiety and the moral distress that may arise when health care workers are prevented from treating patients or protecting them from harm as a result of seeking medical care 55 56. Clinicians should refer to their institution's policies regarding interactions with law enforcement and consult legal counsel rather than individually respond to immigration-enforcement activities in health care settings.
The American College of Obstetricians & Gynecologists opposes policies that require documentation of immigration status in the medical record. Clinicians should not seek or document information that may put a patient at legal risk, especially when the information is not clinically relevant to the care plan. Unless mandated by law, health care professionals should document only information related to a patient's migration history that is necessary for the ongoing clinical care 57 58. Clinicians who are required to document sensitive and private patient information that compromises patient safety are at risk of developing moral distress 59.
The American College of Obstetricians & Gynecologists encourages hospitals and other health care institutions to proactively develop policies on interactions with federal immigration and other law enforcement officials to guide clinicians and staff.
Despite the rescission of protection of health care spaces as “sensitive locations,” health care institutions must continue to comply with Health Insurance Portability and Accountability Act (HIPAA) regulations. Health system leaders should review and update policies on access to protected health information and create clear policies regarding interactions with immigration and other law enforcement officials 61 and work with their institutions to create clinical spaces that are welcoming to immigrants (eg, multilingual signage). System-wide changes can include the identification of public and private spaces within health care settings and the development or revision of institutional policies on immigration enforcement, the confidentiality of patient information, and refraining from the documentation of patients' immigration status 59. Obstetrician–gynecologists should engage in team-based education about how to create welcoming and safe settings. Setting expectations about the U.S. health care system and addressing health literacy gaps (eg, explanations of visits, the role of pharmacies and other ancillary services, and how to manage a medical emergency) may be particularly helpful for immigrants who may have differing experiences and expectations of the health care system. Trauma-informed approaches 64, screening for mental health conditions, recognition of possible human trafficking 65, and empathy for immigration-related stressors are important for building patient–clinician trust. When patients share concerns related to their immigration status, clinicians should provide reputable medical–legal resources (such as family-preparedness planning for mixed-status families) or referrals to trusted community partners Box 1. Health care professionals can practice cultural humility and responsiveness by incorporating family norms about medical decision making and affirming traditional forms of healing, as long as they are not known to be harmful to health. Mitigating clinician bias that may manifest in hierarchical decision making, poor communication, rushed visits, delays in care, or other forms of differential treatment of immigrant patients also is important to make immigrants feel welcome in health care settings 66. Obstetrician–gynecologists are encouraged to work with their system leaders to support enhanced language access for patients who communicate in languages other than English 67. See other ACOG resources for additional information on the importance of language-concordant clinicians, the role of certified medical interpreters, and how to assess health literacy and understanding, especially when an interpreter is present 67 68 69.
Obstetrician–gynecologists should promote and support research that monitors the effects of restrictive immigration policies on health care access, utilization, quality, patient experiences, and outcomes.
Box 1.
Resources
Doctors for Immigrants(https://doctorsforimmigrants.com/)
“Welcoming and Protecting Immigrants in Healthcare Settings: A Toolkit Developed from a Multi-State Study” (https://doctorsforimmigrants.com/wp-content/uploads/2020/01/WelcomingProtectingImmigrants-toolkit-3.pdf) provides actions to implement change at the institutional, clinician, and patient levels, including training strategies and educational tips plus sample policies and scripts.
National Immigration Law Center (NILC)(https://www.nilc.org/)
The NILC provides information for health care professionals on how to prepare for and respond to enforcement actions by immigration officials and interactions with law enforcement, including “Health Care Providers and Immigration Enforcement: Know Your Rights, Know Your Patients' Rights” (https://www.nilc.org/resources/healthcare-provider-and-patients-rights-imm-enf/).
American Civil Liberties Union (ACLU)(https://www.aclu.org/)
The ACLU provides information (https://www.aclu.org/documents/health-care-providers-guide-best-practices-protecting-your-rights-and-your-patients-rights) for hospitals, medical centers, community health centers, other health care facilities, health care professionals, medical associations, and advocates on how to prepare for and respond to enforcement actions by immigration officials, interactions with law enforcement that could result in immigration consequences for their patients, and law enforcement presence that deters access to care.
Immigrant Legal Resource Center (ILRC)(https://www.ilrc.org/)
The ILRC offers a variety of resources, including Red Cards/Tarjetas Rojas (https://www.ilrc.org/red-cards-tarjetas-rojas) that provide examples of people's rights and protections under the U.S. Constitution regardless of immigration status and a fillable and printable “Step-by-Step Family Preparedness Plan” (https://www.ilrc.org/resources/step-step-family-preparedness-plan).
Health Begins(https://healthbegins.org/immigration-enforcement-in-healthcare-settings-how-to-prepare-and-respond/)
This site provides resources and guidance to address how health care partners can prepare for potential U.S. Immigration and Customs Enforcement encounters on their premises and respond in the interim to concerns among patients and staff.
Research evaluating the effects of restrictive immigration policies on reproductive health outcomes is essential, especially for policy makers seeking evidence-based solutions to health inequities. Barriers to research include limitations on funding priorities, access to datasets, and methods to safely identify immigrants who may avoid participating in research studies based on concerns related to their immigration status 70. Research also is needed to evaluate the effects of punitive immigration laws and policies on health care workers, including moral injury on clinicians and career burnout 71. Additionally, recent changes to the H-1B visa program hold the potential for limiting health care access by blocking health care professionals from other countries from working in the United States. Beyond the walls of academic medicine, obstetrician–gynecologists can collaborate with social science researchers, community members, grassroots organizations, medical–legal teams, and other collaborators to foster robust research on the effects of restrictive immigration policies on health care access.
The American College of Obstetricians & Gynecologists recommends that obstetrician–gynecologists take an active role in local, state, regional, and national advocacy efforts to improve health care access and quality, regardless of immigration status.
As experts in the harms that women and gender-diverse individuals experience as a result of exclusionary immigration and health policies, obstetrician–gynecologists are uniquely positioned to advocate for patients at the individual, institutional, state, and national levels. They can join in collective action with local, grassroots advocacy organizations, as well as professional societies. Collective action can include fundraising; signing petitions or letters; writing to legislators; writing op-eds for the public; and participating in press conferences, media interviews, and rallies. Advocacy training is helpful in building skills to communicate public narratives to different audiences.
Conclusion
The American College of Obstetricians & Gynecologists supports the health and well-being of all individuals seeking obstetric and gynecologic care, regardless of immigration status. Access to timely and evidence-based health care should be provided for those held in immigration detention facilities; individuals who are pregnant should not be targeted for immigration enforcement. Health care institutions should provide robust guidance and support for health care personnel and patients faced with the continued complexities of the dynamic landscape of immigration policies. Obstetrician–gynecologists should advocate for the unique needs of patients who are immigrants to promote reproductive justice and health equity.
Use of Language
ACOG recognizes and supports the gender diversity of all patients who seek obstetric and gynecologic care. In original portions of this document, authors seek to use gender-inclusive language or gender-neutral language. When describing research findings, this document uses gender terminology reported by investigators. To review ACOG's policy on inclusive language, see https://www.acog.org/clinical-information/policy-and-position-statements/statements-of-policy/2022/inclusive-language .
Conflict of Interest Statement
All ACOG committee members and authors have submitted a conflict of interest disclosure statement related to this published product. Any potential conflicts have been considered and managed in accordance with ACOG's Conflict of Interest Disclosure Policy. The ACOG policies can be found on acog.org . For products jointly developed with other organizations, conflict of interest disclosures by representatives of the other organizations are addressed by those organizations. The American College of Obstetricians & Gynecologists has neither solicited nor accepted any commercial involvement in the development of the content of this published product.