Number 20
This Committee Statement was developed by the American College of Obstetricians & Gynecologists’ Committee on Ethics in collaboration with Colleen Denny, MD, and Mara Greenberg, MD.
ABSTRACT: The term “telehealth” is used to describe technology-enhanced health care frameworks that allow traditional clinical diagnosis and monitoring to be delivered or facilitated by technology. The terms “telemedicine,” “connected health,” and “digital health” are also used to describe similar technological applications in health care. These frameworks may include services such as virtual visits, remote patient monitoring, and mobile health care. Relying on the core ethical principles can assist obstetrician–gynecologists in ethical conduct or interpretation of these novel technologies as they arise. In this Committee Statement, we discuss the ethical implications and relevant questions involved in the increasing adoption of telehealth in obstetrics and gynecology and how best to ensure that these new modalities align with the foundational bioethical principles of beneficence, nonmaleficence, autonomy, and justice.
Summary of Recommendations and Conclusions
On the basis of the principles outlined in this Committee Statement, the American College of Obstetricians & Gynecologists (ACOG) offers the following recommendations and conclusions:
ACOG supports the use of telehealth care models to improve the quality of and increase access to obstetric and gynecologic care.
Telehealth should be supported as an appropriate alternative to in-person care when necessary, safe, and effective care delivery can be achieved through this modality.
Obstetrician–gynecologists using telehealth must establish clear protocols to identify signs or symptoms that should be followed up in person and accordingly direct patients toward appropriate, timely follow-up evaluation.
Obstetrician–gynecologists should provide targeted patient support for the initiation and continuation of telehealth that is responsive to individuals' needs and values.
Obstetrician–gynecologists offering telehealth should use software, products, and practice patterns specifically designed for such visits to ensure data security and privacy.
The decision to use telehealth, in-person care, or a hybrid model of care including both modalities should incorporate shared decision making and consider risks, benefits, health care professional availability, and patient preferences.
Patients should not be unduly pressured to adopt telehealth, and entirely in-person care should be available as an alternative whenever possible.
Obstetrician–gynecologists must be conscious of systemic barriers and choose telehealth modalities that minimize them, including considerations of language fluency and literacy.
Patient-eligibility criteria for telehealth must be considered carefully to avoid excluding patients for operational or logistical reasons who might otherwise be appropriate candidates.
Obstetrician–gynecologists and health care systems have a responsibility to minimize barriers to all clinically appropriate telehealth modalities, including barriers posed by reimbursement disparity.
If evidence continues to support the benefits of telehealth, it becomes increasingly incumbent on obstetrician–gynecologists to self-educate and adopt in accordance with the needs of their patient population.
Background
The term “telehealth” is used to describe technology-enhanced health care frameworks that allow traditional clinical diagnosis and monitoring to be delivered or facilitated by technology. The terms “telemedicine,” “connected health,” and “digital health” are also used to describe similar technological applications in health care. These frameworks may include such services as virtual visits, remote patient monitoring, and mobile health care 1.
In the field of obstetrics and gynecology, telehealth may refer to models of health care for a given condition in which aspects of health care, such as evaluation, counseling, and follow-up, are enabled through technology. Hybrid models of prenatal care, in which pregnant patients alternate between visits in a traditional health care facility and virtual visits from home, is a common example of a telehealth-facilitated model of care 3 or smartphone software applications focused on such gynecologic concerns as fertility tracking or premenstrual symptom management 4. These individual telehealth models, devices, or software applications often are updated or replaced rapidly as new approaches and technological capabilities emerge.
Obstetrics and gynecology as a health care field historically has been less likely than other fields in medicine to use telehealth to connect with and care for patients. Before the coronavirus disease 2019 (COVID-19) pandemic, only 9–12% of surveyed obstetrician–gynecologists reported that they used telehealth for physician-to-patient interactions, lower than almost all other medical specialties 5 1, as well as the start-up barriers posed by new equipment and technology needs, especially for smaller practices 5 8 9 10 11. In the wake of the pandemic, many obstetrician–gynecologists are considering which telehealth modalities to continue long-term, how best to implement them, and how telehealth is perceived by patient populations. As with all developments in health care, rapid adoption of new telehealth interventions has the potential to outpace both evidence-based practices and full consideration of the ethical issues involved in using telehealth for obstetric and gynecologic patient care.
As Chaet et al 12 state in their discussion of the ethical implications of telehealth, “While new technologies and new models of care continue to emerge, physicians' fundamental ethical responsibilities do not change…The task is to understand how these fundamental responsibilities may play out differently in the context of telehealth and telemedicine than they do in in-person patient-physician interactions.” Relying on the core ethical principles outlined in this document may assist obstetrician–gynecologists in ethical conduct or interpretation as these novel technologies arise. In this Committee Statement, we discuss the ethical implications and relevant questions involved in the increasing adoption of telehealth in obstetrics and gynecology and how best to ensure that these new modalities align with the foundational bioethical principles of beneficence, nonmaleficence, autonomy, and justice 13.
Ethical Issues and Considerations
Beneficence
Beneficence is described as the duty of health care professionals to act in ways that benefit their patients and to take positive steps to prevent and remove harm from their patients 13. In the context of obstetric and gynecologic care, any analysis of the beneficence of telehealth must consider the demonstrated and theoretical potential for telehealth modalities to benefit patients, in terms of direct health benefits as well as logistic and financial benefits related to nonhealth resources. A growing body of recent research shows the potential for telehealth to provide concrete benefits for patients seeking a wide range of health care services 14. These telehealth interventions may improve outcomes by allowing more frequent engagement with patients, promoting healthy habits, improving patient education, lowering logistical barriers for patients to engage with care, or even improving the accuracy of patient-collected data by using remote devices to send clinical information directly to the physician 15. ACOG supports the use of telehealth care models to improve the quality of and increase access to obstetric and gynecologic care.
In the context of prenatal care, research shows the potential for telehealth to improve asthma control for pregnant patients 16, assist with smoking cessation during pregnancy 14 17 18 19, manage diabetes during pregnancy 14, and monitor patients with hypertension who are at risk of progression to preeclampsia 20. Models of prenatal care that incorporate both telehealth and in-person visits also may be particularly beneficial for patients 22 and promotes breastfeeding continuation 23 24.
In the context of gynecologic care, telehealth interventions have been demonstrated to improve contraception-continuation rates for both the oral contraceptive pill 25 and depot medroxyprogesterone acetate 26 and may present fewer logistical barriers for patients seeking an initial prescription for contraception 27. Patients with stress urinary incontinence significantly benefit from telehealth mobile applications providing patient education and guiding pelvic floor exercises 28, and telehealth models for medication abortion have been shown to maintain high rates of safety and efficacy without requiring in-person assessment 29.
Furthermore, research shows high levels of patient satisfaction with many obstetric and gynecologic telehealth care models. Patients who received a wide range of obstetric and gynecologic care report high satisfaction with telehealth models and interventions, including hybrid prenatal care visit schedules 30 31 32, surgical consultation from female pelvic medicine and reproductive surgery specialists 33, and medication abortion using telehealth 29. Patients who are satisfied with their care are more likely to remain engaged with care going forward, with the potential for longer-term benefits.
Aside from directly improving clinical outcomes, telehealth models and interventions also promote beneficence by allowing patients to receive high-quality health care without physically presenting to a health care facility. Although this aspect often is described as patient “convenience,” by taking the place of some or all traditional in-person health care visits, telehealth may decrease significant financial and logistical burdens for patients seeking care, such as the needs for patients to take time off of work or school, to arrange childcare, or to pay for and coordinate transportation 34 35 36 37 38. These logistical and financial benefits of telehealth may be most salient for patients with limited resources or less accommodating schedules or both and for those seeking types of care not available in person in their home regions 35 39. Transgender and neurodivergent individuals who might have had poor past experiences with in-person care and other patients with aversions to in-person care also may prefer and perceive fewer barriers with virtual care models 40.
Beyond these individual benefits, there is also potential for telehealth models and interventions to provide population-based benefits and to protect the health of the community overall. Although the principle of beneficence traditionally concerns benefits that directly accrue to the individual patient involved in the intervention, these population-level benefits intersect with the principles of communitarian ethics, which focus on the importance of the community and emphasize the influence the community has on individual human beings 34. Greater use of telehealth in appropriate clinical scenarios also respects the nature of in-person assessment as a finite resource in the community. In-person clinical care requires physical health care facility space, staff, and health care professional time, and the judicious use of telehealth allows these resources to be distributed more fairly among patients for whom the need for in-person care is greatest.
Nonmaleficence
Nonmaleficence is the principle that the health care team is obligated to avoid harm to patients 13. When presented with the opportunity to provide telehealth services as an alternative or complementary strategy to in-person care, physicians and patients may experience concerns regarding insufficient ability to achieve care quality, efficacy, and equity; interpersonal and systemic trust; and security of protected and vulnerable health information.
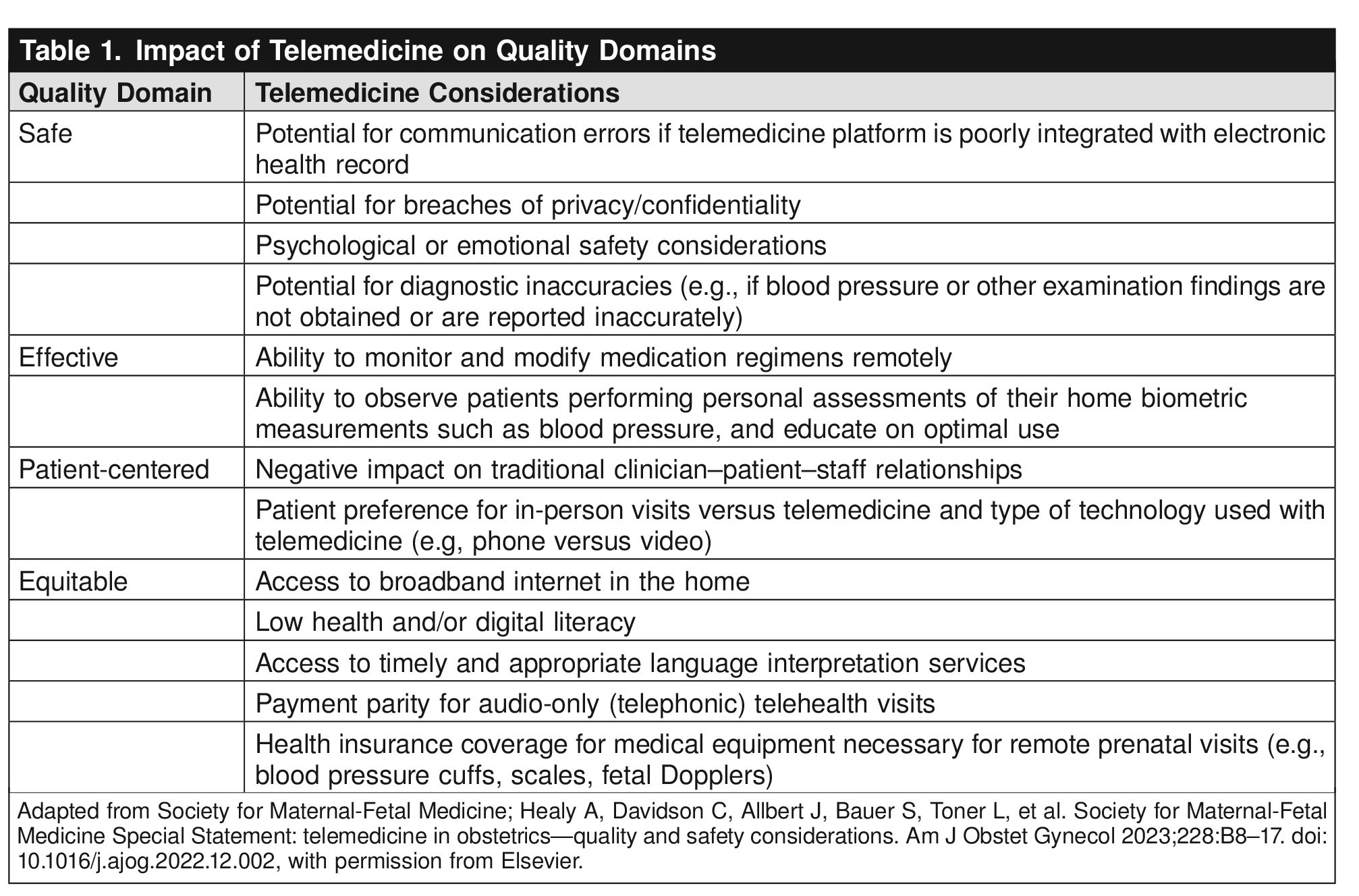
In a 2023 Special Statement on telemedicine quality and safety (42), the Society for Maternal-Fetal Medicine cited the potential for negative effects on several quality domains (of those proposed by the National Academy of Medicine in 2001), that should be considered in avoiding harm when providing telehealth Table 1.

Care Quality and Safety
As a result of widespread incorporation of telehealth into obstetric and gynecologic care during the COVID-19 pandemic, many publications have cataloged adequate telehealth outcomes in comparison with contemporary or historic control groups 43 44 45 46 47 48, as referenced in the Beneficence section above. Despite the results of this natural experiment, in addition to telehealth care quality reviews conducted before the pandemic 14 29, health care professionals must ensure the presence of care standards for telehealth that can maintain and enhance quality, equity, and confidence in this care modality 49 50. Determining which aspects of a patient’s history, vital signs, and examination are necessary for meeting the standard of care during a visit is a key step in ensuring care quality 1 35. Clear communication regarding these standards can counteract the vague sense among physicians and patients that physicians will “miss” important information that can be gathered only during a face-to-face encounter 8 51 52.
Similarly, there is a risk when providing telehealth as an alternative to in-person visits that recommended diagnostic and treatment options may be skewed toward those options that can be achieved without an in-person evaluation or procedure 27 35. This creates a potential for more evidence-based and high-quality options to be de-emphasized or missed altogether. For example, telehealth focused on providing contraception may underemphasize the potential benefits of long-acting reversible contraception, which requires in-person placement.
Finally, patients may disclose concerning information or have concerning findings that cannot be adequately assessed immediately during the telehealth encounter 35. Telehealth should be supported as an appropriate alternative to in-person care when necessary, safe, and effective care delivery can be achieved through this modality. In addition, obstetrician–gynecologists using telehealth must establish clear protocols to identify signs or symptoms that should be followed up in person and accordingly direct patients toward appropriate, timely follow-up evaluation.
Trust and Security
Traditional clinical relationships, trust, and personal health data security are at risk of compromise when incorporating telehealth modalities into clinical care. As a result, telehealth options may not be universally appealing nor trustworthy from a patient perspective 8 42 53 54 55 56, leading some patients to avoid care entirely if they perceive that their only options for receiving care are through telehealth. Patient-centered care engendering satisfaction and trust stems from efforts to respect and respond to individuals’ needs and values and to adapt these efforts to the care modality employed.
Some risks specific to telehealth provision stem from the fact that technology-assisted conveyance of patient information may be uniquely vulnerable from a data privacy or security perspective. Additionally, patients may experience discomfort or mistrust with use of technology based on personal privacy and security concerns. Health care professionals offering telehealth should use software, products, and practice patterns specifically designed for such visits to ensure data security and privacy. However, health care professionals also should strive to be aware of third-party applications or software that patients may choose to engage with independently, such as menstrual tracking applications, and discuss potential security concerns with patients. Finally, limiting or identifying all parties present in telehealth encounters may be more challenging without a defined physical clinical space. These risks may be particularly burdensome for patients seeking personally or logistically sensitive reproductive health care, including sexual health issues or abortion care. In sum, obstetrician–gynecologists should provide targeted patient support for the initiation and continuation of telehealth that is responsive to individuals’ needs and values. Tools to combat trust and security concerns in the provision of telehealth include those outlined in ACOG Committee Opinion No. 798, Implementing Telehealth in Practice 1, and elsewhere 57 58 Box 1.
Box 1.
Supporting Trust and Security in Telehealth
Practice support: Preparation to provide appropriate telehealth services, including:
Obtaining necessary technology resources and equipment and ensuring readiness
Educating providers on avoiding security and privacy violations
Confirming a quiet, professional environment for the care provider
Patient support
Before and at the start of a telehealth visit, describe the intent of the visit and ensure that the patient is prepared to proceed, especially for patients less familiar with telehealth
Document all parties participating in or listening to a telehealth visit, including clinical staff
Explicitly obtain the patient’s permission if a telehealth visit is being recorded
Assess needs of the individual patient regarding telehealth modalities and choose modalities that meet those needs
Use synchronous modalities such as video visits to foster patient–provider relationships and allow real-time data capture
Conversely, for patients who have more concerns about use of video, providers should consider telehealth alternatives to video conferencing
Audio only
Text-based communication, synchronous or asynchronous
Provide patient tips and tools for using their technology in a private and comfortable manner, such as instructions on how to blur the background on video
Alternate care delivery method available:
If a provider cannot ensure the privacy of sensitive health information conveyed by telehealth (eg, information on interpersonal violence, sex trafficking, abortion, or sexually transmitted infection history), it may be ethical to preferentially schedule in-person evaluations to ensure privacy
Autonomy
Respect for autonomy refers to health care professionals' ethical obligation to support and respect patients in making decisions about their own care, including working to prevent limitations, including inadequate understanding, that undermine meaningful choice 13. In the context of telehealth, respect for autonomy includes questions about how patients engage with different modalities of telehealth, as well as whether to use telehealth in the first place.
For a number of reasons, patients may prefer and elect for in-person care when health care professionals believe that telehealth would be equally effective or even superior. These reasons, as described in the Nonmaleficence section, may include general discomfort with or distrust of new technology as well as concerns about confidentiality, including decreased privacy from family members or colleagues in the location where the patient initiates the remote visit or the security of the technology platform itself 37 58 59 60.
Alternatively, patients may prefer telehealth or decline in-person evaluation even when health care professionals recommend face-to-face care. These preferences may be secondary to logistical challenges in presenting for in-person care; financial concerns 61; stigma associated with reproductive health care 62; or health-related apprehensions, including infectious disease exposure 58.
The decision to use telehealth, in-person care, or a hybrid model of care including both modalities should incorporate shared decision making and consider risks, benefits, health care professional availability, and patient preferences. This process involves ongoing patient education, patient support, and engagement with affected patient communities. Health care professionals should share information about the potential benefits and limitations of telehealth with patients before initiation of telehealth and during individual telehealth visits and interactions 63. Obstetrician–gynecologists using telehealth modalities for patient care should provide targeted patient support for the initiation and continuation of telehealth, such as tipsheets for patients 65.
Patients still may have persistent concerns and choose to decline telehealth despite optimal education, support, and diligence on the part of obstetrician–gynecologists. Patients should not be unduly pressured to adopt telehealth, and obstetrician–gynecologists should support patients’ choices by offering entirely in-person care as an alternative whenever possible.
Obstetrician–gynecologists also should recognize that patient preferences regarding telehealth may change over time. Data suggest that increased patient-reported satisfaction with telehealth is positively correlated with previous exposure to telehealth and that patients who have used telehealth previously are more likely to choose it again 66 67. Furthermore, specific telehealth platforms and devices evolve rapidly, often in response to patient-usability feedback. A telehealth option that a patient initially declines may become more acceptable as that option develops new features or functionality. Obstetrician–gynecologists should reassess patients’ preferences regarding telehealth modalities periodically and update care plans as indicated.
Justice
Justice in health care represents complex concepts of ensuring equity across many domains, from equitable treatment of individuals to equitable allocation of health care benefits and burdens across societal groups and institutions 13. As discussed in ACOG Committee Opinion No. 390, Ethical Decision Making in Obstetrics and Gynecology, the complexity of achieving justice involves not only clinicians’ obligations to render to patients what is due to them, but also with the health care system’s role in the allocation of limited medical resources in the broader community 68.
When considering the effect on justice of incorporating telehealth into medical practice, we must consider both potential benefits and potential harm 63. Telehealth may increase access to medical care for patients for whom in-person evaluation is particularly burdensome (see Beneficence section). Telehealth can allow specialists to treat and evaluate patients for whom in-person evaluation would not be convenient nor even feasible (those in rural settings or where specialists are rare or where some gynecologic care is stigmatized, such as abortion or contraception care) 39 69 70 71. Multiple publications and reviews support the concept of increased access to care for vulnerable groups and those seeking sensitive care when telehealth is implemented as an alternative to or as an integrated option alongside in-person care.
Telehealth modalities also may be preferentially targeted toward and more easily accessible to patients from more privileged backgrounds, however. Wealth, technology experience, broadband or cell access, home privacy and other circumstances, and language fluency and literacy can lower or create barriers to the use of telehealth 9 60 72. Unequal availability and adoption of telehealth has the potential to exacerbate existing disparities by preferentially increasing the ability of privileged patient groups to access health care professionals more easily and more frequently. Research has identified that patient groups that traditionally face greater barriers in accessing health care also use telehealth relatively less frequently, even with the surge in telehealth rollouts during the COVID-19 pandemic. Non-White patients, patients with no insurance or public insurance 73 74 75, older patients, non–English-speaking patients, and patients with lower income 76 77 are less likely to use telehealth modalities when compared with White, younger, wealthier peers in the same regions and health systems. Further, identification of patients or groups who are at risk of underutilization or suboptimal care receipt when using telehealth modalities is not always straightforward. Even when patients are able to access telehealth and view it as beneficial, they may harbor concerns about being unable to express themselves well using telehealth 78. Obstetrician–gynecologists must be conscious of systemic barriers and choose telehealth modalities that minimize them, including considerations of language fluency and literacy.
A 2021 scoping review of patient-centered outcomes research identified that, “…the most effective health system- and provider-level telehealth implementation solutions to address disparities employ patient-centered and culturally tailored telehealth solutions whose development is actively guided by the patients themselves to meet the needs of specific communities and populations.” 79 Specific best practices in telehealth implementation cited include telehealth provision through trusted intermediaries, close partnership with payers to facilitate reimbursement and sustainability, and practices that support patient-guided confidential sharing of personal health information 79. Pursuing equity in telehealth implementation centers on choosing telehealth modalities, platforms, and standards for conducting telehealth visits that are concordant with the needs of individuals and minimize barriers to uptake. Patient-eligibility criteria for telehealth must be considered carefully to avoid excluding patients for operational or logistical reasons who might otherwise be appropriate candidates. The ability of health care practices to achieve this can be aided by incorporation of community and patient input into the choice and usage of telehealth options 80. Further, health care professionals as consumers can support the development of telehealth platforms that diminish inequities, such as preferentially using software available in multiple languages.
Reimbursement is also a systemic issue that creates barriers to achieving justice in care delivery. According to a 2021 commentary by Ukoha et al 81, payment parity, which constitutes equal reimbursement for remote and in-person visits, is a measure that can combat financial disincentive to offer telehealth and is required to ensure equitable and widespread access. However, even when state programs adopt payment parity, community health centers still may experience lower reimbursement for remote visits and different telehealth modalities that provide the same care may be reimbursed differently. Lower reimbursement for audio-only visits may exacerbate disparities that stem from the “digital divide” created by differential technology access and literacy levels. In addition, regulatory, licensing, and payment policies often are based on face-to-face encounters, rendering parity payment laws potentially inadequate to fulfill the required coding elements in a virtual setting 1 82. Lack of payment parity between in-person and virtual care may particularly threaten hybrid models of care in which the same health care team and facility provides both types of care.
Reimbursement models should recognize the existence of such barriers to avoid disincentivizing obstetrician–gynecologists from offering telehealth to patients without broadband access or without more advanced technology available to them. Obstetrician–gynecologists and institutions should advocate for improved reimbursement parity models that recognize the value of clinician time and counseling complexity rather than focusing only on the physical setting of care. Obstetrician–gynecologists and health care systems have a responsibility to minimize barriers to all clinically appropriate telehealth modalities, including barriers posed by reimbursement disparity.
Finally, in aspiring to achieve justice in reproductive health care, we must consider whether obstetrician–gynecologists have an obligation to adopt telehealth into their practices. Adoption of innovative practices is integral to medical progress and simultaneously poses ethical challenges to patient safety and autonomy as outlined above. Clinician obligations with respect to these concepts are described in ACOG Committee Opinion No. 352, Innovative Practice: Ethical Guidelines 83. Furthermore, obstetrician–gynecologists considering how to incorporate telehealth may be limited by evolving political and regional regulations; states may have important restrictions on how and where telemedical care can be conducted, and health care professionals should familiarize themselves with relevant state laws and regulations. Similar to the historical adoption of other new practice models and technologies, such as minimally invasive surgery, practitioners of obstetrics and gynecology should assess burdens and requirements of telehealth incorporation with the same balance of expediency and caution. If the evidence continues to support the benefits of telehealth, it becomes increasingly incumbent on obstetrician–gynecologists to self-educate and adopt in accordance with the needs of their patient population.
Conclusion
The rapidly evolving landscape surrounding the ethical provision of telehealth provides many opportunities for obstetrician–gynecologists to provide benefits, reduce harms, and elevate person-centered, equity-focused care in ways that enhance and supersede traditional care models. New telehealth care models will continue to emerge and evolve, and obstetrician–gynecologists must adhere to foundational ethical principles when considering how best to integrate these models into their practices. Barriers to appropriate telehealth adoption require an educated and forward-thinking approach from individual obstetrician–gynecologists, health care systems, and societal institutions, which must be flexible enough to adapt as technology and patient needs change while remaining grounded in ethical principles outlined above.
Use of Language
The American College of Obstetricians & Gynecologists (ACOG) recognizes and supports the gender diversity of all patients who seek obstetric and gynecologic care. In the original portions of this document, authors seek to use gender-inclusive language or gender-neutral language. When describing research findings, this document uses gender terminology reported by investigators. ACOG's policy on inclusive language can be reviewed at https://www.acog.org/clinical-information/policy-and-position-statements/statements-of-policy/2022/inclusive-language.
Conflict of Interest Statement
All ACOG committee members and authors have submitted a conflict of interest disclosure statement related to this published product. Any potential conflicts have been considered and managed in accordance with ACOG's Conflict of Interest Disclosure Policy. The ACOG policies can be found on acog.org. For products jointly developed with other organizations, conflict of interest disclosures by representatives of the other organizations are addressed by those organizations. The American College of Obstetricians & Gynecologists has neither solicited nor accepted any commercial involvement in the development of the content of this published product.