Number 14
This Committee Statement was developed by the American College of Obstetricians and Gynecologists' Committee on Advancing Equity in Obstetric and Gynecologic Health in collaboration with Torie Comeaux Plowden, MD, MPH, Natalie Whaley, MD, MPH, and Alicia Christy, MD, MHSCR.
ABSTRACT: Diagnostic testing and treatment for infertility should be available to everyone in need of these services. The disparities in rates of infertility and the barriers to accessing assisted reproductive technology services should be understood through and addressed within a reproductive justice framework. Obstetrician–gynecologists and other health care professionals should identify specific populations at risk and their accompanying barriers to access to help improve infertility care across populations. Health care professionals should ask appropriate questions about social and structural drivers of health that may influence a patient’s health and use of the health care system to better understand their patients’ needs and lived experiences. Obstetrician–gynecologists and other health care professionals should advocate for insurance coverage for infertility services, including assisted reproductive technology; policy changes that promote comprehensive reproductive health; and evidence-based, lower cost treatment options.
Recommendations and Conclusions
Based on the principles outlined in this Committee Statement, the American College of Obstetricians and Gynecologists (ACOG) makes the following recommendations and conclusions regarding infertility in historically and intentionally excluded communities:
Patients with infertility have a medical disease (not a “social condition”), and health care professionals should provide medically and ethically sound care specific to the etiology of a patient’s diagnosis.
Obstetrician–gynecologists should ask all patients about reproductive planning and attempts at pregnancy.
Obstetrician–gynecologists and other health care professionals should understand the circumstances in which immediate referrals to subspecialists in reproductive endocrinology and infertility are necessary.
Obstetrician–gynecologists and other health care professionals should identify specific populations at risk and their accompanying barriers to access to help improve infertility care across populations.
Obstetrician–gynecologists and other health care professionals should recognize that social determinants of health greatly influence access to care and should strive to identify and mitigate self-bias and systemic barriers to equity in access and care.
Obstetrician–gynecologists and other health care professionals should collaborate with local and national agencies to provide support for individuals diagnosed with infertility.
Obstetrician–gynecologists and other health care professionals should advocate for insurance coverage for infertility services, including assisted reproductive technology, policy changes that promote comprehensive reproductive health, and evidence-based lower cost treatment options.
Obstetrician–gynecologists and other health care professionals should intentionally provide patient education about fertility and infertility.
Continued research is needed to identify strategies to improve outcomes for individuals with infertility, especially in communities with barriers to access to infertility services.
Background
Diagnostic testing and treatment for infertility should be available to everyone in need of these services. Yet, many individuals do not have access to this necessary care. Various issues limit access to appropriate treatment, including economic barriers. Only recently has infertility been recognized more universally as a medical condition. As defined by the American Society for Reproductive Medicine (ASRM), infertility is the “result of a disease (an interruption, cessation, or disorder of body functions, systems, or organs) of the male or female reproductive tract which prevents [pregnancy] or the ability to carry a pregnancy to delivery” 2.
Disparities exist not only in access to services, but also in the prevalence of infertility. The Centers for Disease Control and Prevention estimates that 19% of married women aged 15–49 years with no prior births have infertility (they are not surgically sterile and are unable to achieve pregnancy after 1 year of trying). Approximately 16% of currently married women aged 15–49 years have difficulty achieving pregnancy or carrying a pregnancy to term (impaired fecundity) 3. This statistic does not include the many single women and members of the LGBTQ+ community who will require medical assistance to procreate.
Some studies have shown that individuals in some racial and ethnic groups are more likely to experience infertility. A cross-sectional analysis of women aged 33–44 years found that Black women had twofold increased odds (95% CI, 1.3–3.1) of infertility when compared with White women after adjustment for socioeconomic status, pregnancy intent, and risk factors for infertility 4. Additionally, difficulty paying for services was associated with infertility among Black women but not White women.
Although the literature is limited, Asian American patients are more likely to experience infertility, wait longer to seek infertility treatment, and have lower success rates compared with White women 5. Some data suggest that, although Hispanic women do not have a higher prevalence of infertility, they have lower rates of use of infertility services when compared with non-Hispanic White women, even after an infertility evaluation 6. A study found that American Indian and Alaska Native female respondents had a 1.37 times greater prevalence of infertility and a 1.3 times greater prevalence of impaired fecundity compared with White women 7. For Black, Indigenous, and people of color, the prevalence of infertility often is high; even when it is comparable with the prevalence in White women, the utilization of infertility services is lower 7. The existing disparities in prevalence of disease and access to needed services are further exacerbated by the current climate of accelerated assaults on reproductive rights.
Reproductive justice, a framework created in the 1990s by Black women, highlights the importance of reproductive autonomy, including the right to become pregnant and the right not to be pregnant, as well as the right to parent one’s children in safe communities 9. The disparities in rates of infertility and the barriers to accessing assisted reproductive technology services should be understood through and addressed within a reproductive justice framework.
Recommendations and Conclusions
Patients with infertility have a medical disease (not a “social condition”), and health care professionals should provide medically and ethically sound care specific to the etiology of a patient’s diagnosis.
Infertility is recognized as a medical condition by multiple international and national organizations, including the World Health Organization, the ASRM, and the American Medical Association 2 10 12. People with infertility should be taken seriously by health care professionals, be treated with compassion, receive an appropriate workup, and participate in a discussion about their treatment options.
Obstetrician–gynecologists should ask all patients about reproductive planning and attempts at pregnancy.
Obstetrician–gynecologists have the unique opportunity to guide their patients through decisions across their reproductive lifespans. The “One Key Question Initiative” acknowledges how one simple question can open a conversation of high importance: “ Would you like to become pregnant in the next year?” 13. This allows an opportunity for a prepregnancy visit and to open a discussion regarding future fertility goals and desires.
Obstetrician–gynecologists and other health care professionals should understand the circumstances in which immediate referrals to subspecialists in reproductive endocrinology and infertility are necessary.
Given that individuals who are trying to become pregnant but have not yet been successful often present to their gynecologist first, it is critically important that obstetrician–gynecologists feel comfortable taking a history, completing a physical examination, and undertaking an infertility workup. Although a patient may be referred to an infertility subspecialist at any time during this process, there are several reasons warranting an immediate referral to a reproductive endocrinologist Box 1.
Box 1.
When an Immediate Referral to a Reproductive Endocrinologist is Warranted
Women older than age 40 years
Patients with the following conditions:
Irregular menstrual cycles, cycle length less than 25 d, intermenstrual bleeding, oligomenorrhea, or amenorrhea
Known or suspected uterine, tubal, or peritoneal disease or endometriosis
Known or suspected male subfertility
Sexual dysfunction
Genetic or acquired conditions that predispose to diminished ovarian reserve (eg, chemotherapy, radiation exposure, FMR1 premutation)
Data from Fertility evaluation of infertile women: a committee opinion. Practice Committee of the American Society for Reproductive Medicine. Fertil Steril 2021;116:1255–65. doi: 10.1016/j.fertnstert.2021.08.038
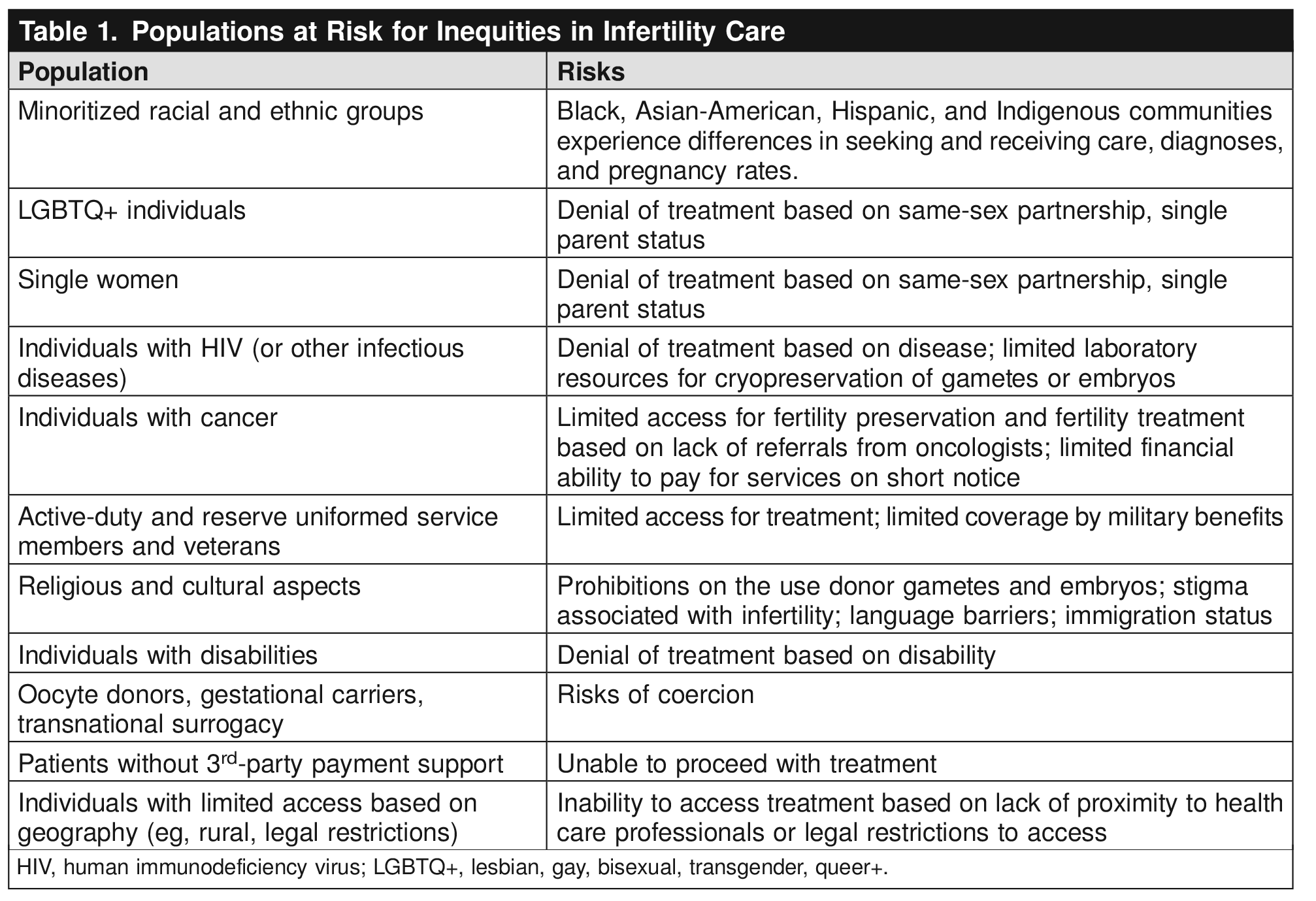
Obstetrician–gynecologists and other health care professionals should identify specific populations at risk and their accompanying barriers to access to help improve infertility care across populations.
Disparities exist in access and treatment outcomes, particularly in Black, Latina, and Native American populations. These disparities extend to other vulnerable groups as well. Health care professionals should be aware of the challenges faced by these specific populations. Members of the LGBTQ+ community and single heterosexual women have been denied treatment in the past, which is against the ASRM’s ethical standards 2 14. Transgender individuals in particular are vulnerable. Due to the potential effects of cross-sex hormone therapy on gonads (particularly on spermatogenesis), all transgender patients should be counseled about fertility preservation before receiving medical treatment 14 15. Individuals with cancer should be offered fertility preservation; depending on their disease status, fertility preservation often may be completed before undergoing gonadotoxic therapy 16. This is of particular importance for adolescents and young people with cancer 17. Additionally, some other diseases (ie, systemic lupus erythematosus and hematologic disorders) also may require treatment with gonadotoxic therapy. Thus, these patients also should be offered fertility preservation 12. Active-duty and reserve uniformed service members and veterans also experience lack of access to care 18. Geographic barriers can impede care, because many infertility clinics are concentrated in urban areas 12. In fact, approximately 18 million reproductive-aged people live in areas without any assisted reproductive technology clinics 19. See Table 1 for a more comprehensive, though not all-inclusive, list of populations at risk for inequities in infertility care.

Obstetrician–gynecologists and other health care professionals should recognize that social determinants of health greatly influence access to care and should strive to identify and mitigate self-bias and systemic barriers to equity in access and care.
A substantial barrier to addressing inequities in infertility care is the internal biases of health care professionals. This can be manifested by health care professionals making clinical assumptions based on personal bias, inappropriate referral patterns, and a failure to become educated about the subject area. Obstetrician–gynecologists and other health care professionals should recognize that making presumptions about a patient’s cultural beliefs can adversely affect their ability to provide appropriate care 20. Furthermore, health care professionals should ask appropriate questions about social and structural drivers of health that may influence a patient’s health and use of the health care system to better understand their patients’ needs and lived experiences 20.
There is a growing body of literature that indicates that systemic racism directly contributes to health disparities 21. Health care professionals should understand the roles that personally mediated, systemic, and structural racism play in creating and perpetuating adverse health outcomes and health care experiences 22. Biases against other vulnerable groups (eg, nonnative English speakers, individuals who are undocumented, and those from nondominant religious groups) also may contribute to disparities in access. Health care professionals should ensure adequate interpreter services when not communicating with patients in their primary language 20. Disparities in infertility care are magnified further because these same groups are disproportionately affected by social determinants of health 23.
Obstetrician–gynecologists and other health care professionals should collaborate with local and national agencies to provide support for individuals diagnosed with infertility.
A notable number of individuals diagnosed with infertility will experience mental health distress. Several studies have found that 30–40% of women undergoing infertility treatment had depression and anxiety 24 25 26 27. Other studies have noted that women with infertility experience shame, grief, a perceived lack of femininity, and self-blame 28 29. A qualitative study revealed five themes among women with infertility experience: 1) anxiety; 2) mood disturbance; 3) threat to self-esteem, identity, and purpose; 4) deterioration of the couple; and 5) weakened support network 30. Health care professionals should be sensitive to potential emotional and psychological issues related to infertility, prepared to support their patients, and aware of national organizations and support groups that cater to individuals with infertility.
Obstetrician–gynecologists and other health care professionals should advocate for insurance coverage for infertility services, including assisted reproductive technology; policy changes that promote comprehensive reproductive health; and evidence-based, lower cost treatment options.
Economic barriers make infertility treatment inaccessible to many, particularly members of Black, Asian-American, Hispanic, and Indigenous communities. The ASRM notes that fertility treatment is, “…available mainly to non-Hispanic Whites and the economic elite…” and that this inequity perpetuates the idea that treatment is a “lifestyle choice” 12. Insurance coverage for infertility care is very limited in the United States, and fewer than half of states have mandated coverage 12. To improve access to care, robust, comprehensive insurance coverage for fertility treatment must be made widely available and health care professionals should seek evidence-based, lower-cost methods of treatment, including strategies to lower the cost of in vitro fertilization (eg, natural cycle or low stimulation cycles). The 2022 Dobbs v. Jackson Women’s Health Organization decision continues to threaten reproductive rights beyond just the right to abortion, and the effects on fertility treatment are still unclear. Obstetrician–gynecologists should advocate for policies that support comprehensive reproductive health, including access to infertility services 32. Although literature regarding infertility is more limited, disparities in health literacy and fertility knowledge are associated with sociodemographic factors. Fertility awareness, in general, is low to moderate among reproductive-aged individuals, with more highly educated individuals having greater fertility awareness 33. Data also suggest that individuals from low-resource, largely immigrant communities who are seeking access to fertility services have greater disparities in fertility knowledge and lower health literacy compared with individuals from high-resource backgrounds 34. Identification and recognition of risk factors for lower health literacy can help inform interventions. One example of changes that can be made is with the reading level of patient-education literature. Despite the fact that most adults read at an 8th-grade level, most health care materials are written at a 10th-grade level or higher 35. Patient materials that are written at an appropriate reading level to be easily understood and that are available in a patient’s native language can help decrease disparities in fertility knowledge.
Continued research is needed to identify strategies to improve outcomes for individuals with infertility, especially in communities with barriers to access to infertility services.
Race and ethnicity data often are missing in studies and registries. Thus, it is likely that disparities in infertility care are underreported. A study of SART CORS data, a population-based analysis of in vitro fertilization cycles, found that race and ethnicity was reported in only 51.6% of cycles 36. To understand disparities and address inequities in infertility care, universal and accurate reporting of race and ethnicity must occur in all research.
Conclusion
Reproduction is a basic human right 12. Improving access and eliminating disparate outcomes regardless of race and ethnicity, geographic location, socioeconomic status, martial status, sexual orientation, or gender identity must be the ultimate goal to attain reproductive justice in America.
Use of Language
ACOG recognizes and supports the gender diversity of all patients who seek obstetric and gynecologic care. In original portions of this document, the authors seek to use gender-inclusive language or gender-neutral language. When describing research findings, this document uses gender terminology reported by the investigators. ACOG's policy on inclusive language can be reviewed at https://acog.org/clinical-information/policy-and-position-statements/statements-of-policy/2022/inclusive-language.
Conflict of Interest Statement
All ACOG committee members and authors have submitted a conflict of interest disclosure statement related to this published product. Any potential conflicts have been considered and managed in accordance with ACOG's Conflict of Interest Disclosure Policy. The ACOG policies can be found on acog.org . For products jointly developed with other organizations, conflict of interest disclosures by representatives of the other organizations are addressed by those organizations. The American College of Obstetricians and Gynecologists has neither solicited nor accepted any commercial involvement in the development of the content of this published product.