

Influenza FAQs for Obstetrician–Gynecologists
Physician FAQ
These FAQs were developed by an assembled work group of practicing obstetrician–gynecologists and ACOG members with expertise in obstetrics, maternal–fetal medicine, infectious disease, and hospital systems. They are based on expert opinion and are intended to supplement the ACOG Practice Advisory Influenza in Pregnancy: Prevention and Treatment. These FAQs may be updated or supplemented to incorporate new data and relevant information as needed.
Looking for patient information? Read The Flu Vaccine and Pregnancy.
Updated October 2025
Frequently Asked Questions
-
Yes. Influenza vaccination is an essential element of prenatal care because influenza can lead to serious illness, including a higher chance of developing pneumonia, when it occurs either in the antepartum or postpartum period.
The American College of Obstetricians and Gynecologists (ACOG) has recently reaffirmed its strong recommendation that all adults receive an annual influenza vaccine and that all women who are or will be pregnant during influenza season should receive any licensed, recommended, age-appropriate, inactivated influenza vaccine during any trimester, as soon as it is available.
Multiple studies indicate that during pregnancy, women are at increased risk of serious medical complications from influenza. In addition, because the influenza vaccine is not effective in infants younger than 6 months, passive immunization of fetuses through transplacentally transmitted antibodies is currently the best prevention strategy for newborns.
Vaccination in the postpartum period is an alternative only when vaccination during pregnancy cannot be completed. It is safe for lactating individuals to receive the flu vaccine.
-
Yes. Numerous studies, including clinical trials and observational studies, along with data from safety reporting systems, have consistently demonstrated the safety of influenza vaccination during pregnancy (Donahue 2019; Panagiotakopoulos 2020; Nordin 2014; Kharbanda 2017). In addition, multiple peer-reviewed studies have repeatedly demonstrated that newborns of women who received the flu vaccine while pregnant have much lower rates of influenza than newborns whose mothers were not vaccinated during pregnancy.
Pregnant women also should be counseled that no scientifically provable or reproducible evidence has been produced to support claims of an association between influenza vaccination during pregnancy and miscarriage (Regan 2023; Regan 2024; Giles 2019; Sperling 2018). In addition, the evidence-based recommendations from the Centers for Disease Control and Prevention (CDC) and other national organizations for the safety of flu vaccine given in any trimester of pregnancy have not changed since the 1990s (CDC 2025; ACIP 1997; Grohskopf 2024; Mackin 2021). The influenza vaccine is made the same way each year, with the only difference being the use of different strains of influenza virus.
-
All women who are or will be pregnant during influenza season, typically September through April, should receive an inactivated influenza vaccine as soon as it is available.
Ideally, influenza vaccination should be given before the onset of influenza circulation in the community, but vaccination at any time during the influenza season is encouraged to ensure protection during the period of circulation. The inactivated influenza vaccine can be given to all women during any trimester.
Because flu vaccines are recommended annually for all adults, pregnant women should be vaccinated even if they received a flu vaccine during a previous pregnancy.
-
Pregnant women should receive any licensed, recommended, age-appropriate inactivated influenza vaccine, given as an intramuscular injection in the deltoid muscle. The American College of Obstetricians and Gynecologists does not preferentially recommend a specific formulation of the influenza vaccine.
-
Egg allergy, including hives, is no longer a contraindication to receipt of the influenza vaccine.
Individuals, including pregnant women, who have experienced only hives after exposure to egg should receive any licensed, recommended, age-appropriate influenza vaccine. Individuals who reported symptoms other than hives (eg, angioedema, respiratory distress, lightheadedness, or recurrent emesis) or who required epinephrine or another emergency medical intervention, also may receive any licensed and recommended influenza vaccine that is otherwise appropriate.
However, their vaccine should be administered in an inpatient or outpatient medical setting and under the supervision of health care professionals who are able to recognize and manage severe allergic conditions. A previous severe allergic reaction to influenza vaccine, regardless of the component suspected of causing the reaction, is a contraindication to future receipt of the vaccine.
-
Yes. Although some individuals have raised concerns that thimerosal, a mercury-containing preservative used in multidose vials of the influenza vaccine, may be unsafe, there is no scientific evidence that thimerosal-containing vaccines cause health or developmental problems, including autism, in children born to women who received vaccines with thimerosal during pregnancy (Price 2010; Thompson 2007; Tozzi 2009; Verstraeten 2003; Stehr-Green 2003).
Of note, no childhood vaccines have contained thimerosal since 2001, and the majority (80%) of the 14 current preparations of influenza vaccine for injection are available in single-dose pre-filled syringes that do not require thimerosal (Immunize.org). Still, based on current evidence, ACOG does not indicate a preference for thimerosal-containing or thimerosal-free vaccines for any group, including pregnant women.
-
ACOG encourages clinicians to stock and ideally, administer all recommended vaccines in their offices. Studies show that immunization rates are higher when a trusted clinician can strongly recommend, offer and administer the vaccine during the same visit, as opposed to recommending vaccination and referring the patient elsewhere to receive the vaccine. Influenza and Tdap vaccines are routinely offered and administered by a majority of practices, while other vaccines are not as commonly stocked, leaving significant gaps in coverage (CDC 2024, O’Leary 2019). When clinicians make immunizations an integral part of their practice and routinely recommend and administer indicated vaccine, they help to increase vaccination rates for pregnant people.
Many obstetrician–gynecologists also perceive a lack of reimbursement as a major barrier to including immunization services in their practices (Leddy 2009). However, with proper documentation and coding, these services can be reported to third-party payers and reimbursement can be received. The practice should adhere to basic coding principles when billing for immunization services. In general, the appropriate vaccine product code should always be reported along with the appropriate Current Procedural Terminology (CPT) vaccine administration code.
For more information on coding, please visit, Immunization Coding for Obstetrician-Gynecologists.
-
Yes. You can give the tetanus toxoid, reduced diphtheria toxoid, and acellular pertussis (Tdap) vaccine, the flu vaccine, the COVID-19 and the RSV vaccine in the same visit. Receiving these vaccinations at the same time is safe and effective and does not impact the protection of any of the individual vaccines.
-
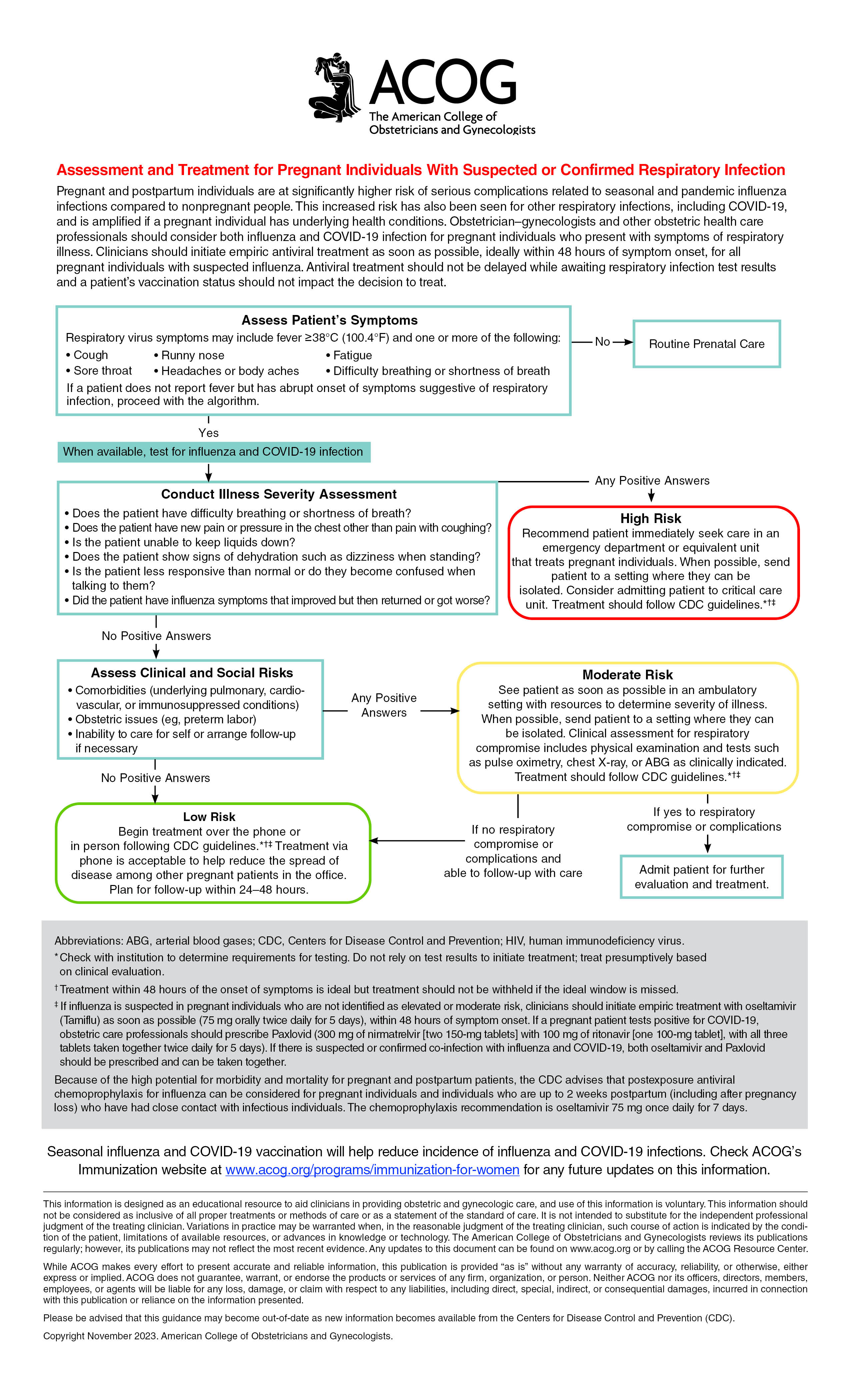
Pregnant women are at high risk of serious complications of influenza infection, such as intensive care unit admission, preterm delivery, and maternal death.
Patients with flu-like illness should be treated with antiviral medications presumptively regardless of vaccination status. Treatment with oseltamivir (75 mg twice daily for 5 days) is preferred; however, if oseltamivir is unavailable, zanamivir (two inhalations [10 mg] twice daily for 5 days) may be substituted (CDC 2023).
Health care professionals should not rely on or wait for test results to initiate treatment for suspected influenza infection and should treat presumptively based on clinical evaluation. For more information on treating suspected influenza, please see ACOG’s algorithm, Assessment and Treatment for Pregnant Women with Suspected or Confirmed Influenza.
-
Obstetrician–gynecologists and other obstetric care professionals should consider both influenza and SARS-CoV-2 infection for pregnant individuals who present with symptoms of respiratory illness.
Pregnant individuals should be assessed based on a variety of symptoms, including but not limited to fever of 100.4 °F or higher, cough, fatigue, headache, and body aches. It is important to note that not all people with influenza infection or another respiratory infection, such as SARS-CoV-2, will develop a fever; therefore, the absence of fever should not rule out an influenza or SARS-CoV-2 diagnosis. Initial triage and treatment by telemedicine are acceptable to help reduce the spread of disease among other pregnant patients in the office. When testing is available, pregnant individuals presenting with symptoms of respiratory illness should be tested for both influenza and SARS-CoV-2 infection.
After symptom assessment, obstetrician–gynecologists and other obstetric care professionals should ask patients questions to help determine the severity of the illness. Pregnant individuals who cannot maintain oral fluid intake, show signs of dehydration, experience difficulty breathing or pain in the chest, or exhibit any signs of obstetric complications are considered moderate or high risk and should be referred immediately to an emergency department or equivalent setting. Pregnant individuals without high-risk symptoms but with comorbidities (eg, asthma) or obstetric issues (eg, preterm labor) or who are unable to care for themselves (eg, unable to tolerate oral intake or obtain prescription medications) are considered moderate risk and should be seen as soon as possible in an ambulatory or triage setting with resources to determine the severity of illness.
For more information on assessing suspected influenza, please see ACOG’s algorithm, Assessment and Treatment for Pregnant Women with Suspected or Confirmed Influenza.
-
Yes. Because of the high potential for morbidity, the CDC and ACOG recommend that postexposure antiviral chemoprophylaxis (75 mg of oseltamivir once daily for 10 days) be considered for pregnant women and women who are up to 2 weeks postpartum (which includes pregnancy loss) who have had close contact with someone likely to have been infected with influenza.
If oseltamivir is unavailable, zanamivir can be substituted (at two inhalations once daily for 10 days) (CDC 2023). All women who are pregnant or in the first 2 weeks postpartum should be counseled to immediately call for evaluation if the early signs and symptoms of influenza infection (eg, a fever greater than 100.0 °F coupled with shortness of breath, syncope, or chest pain) develop.
For more information on antiviral chemoprophylaxis in pregnant and postpartum women, see the CDC website.
{kind=link}
References
-
Centers for Disease Control and Prevention. Flu, Tdap, and COVID-19 vaccination coverage among pregnant women – United States, April 2024. CDC; 2024. Accessed October 15, 2025. https://www.cdc.gov/fluvaxview/coverage-by-season/pregnant-april-2024.html
-
Centers for Disease Control and Prevention. Influenza vaccine safety considerations during pregnancy or while breastfeeding. CDC; 2025. Accessed August 20, 2025. https://www.cdc.gov/flu/hcp/vax-summary/vaccine-safety-pregnant.html
-
Centers for Disease Control and Prevention. Influenza antiviral medications: summary for clinicians. CDC; 2023. Accessed August 19, 2025. https://www.cdc.gov/flu/hcp/antivirals/summary-clinicians.html
-
Donahue JG, Kieke BA, King JP, Mascola MA, Shimabukuro TT, DeStefano F, et al. Inactivated influenza vaccine and spontaneous abortion in the Vaccine Safety Datalink in 2012-13, 2013-14, and 2014-15. Vaccine 2019;37:6673–81. doi: 10.1016/j.vaccine.2019.09.035
-
Giles ML, Krishnaswamy S, Macartney K, Cheng A. The safety of inactivated influenza vaccines in pregnancy for birth outcomes: a systematic review. Hum Vaccin Immunother 2019;15:687–99. doi: 10.1080/21645515.2018.1540807
-
Grohskopf LA, Ferdinands JM, Blanton LH, Broder KR, Loehr J. Prevention and control of seasonal influenza with vaccines: recommendations of the Advisory Committee on Immunization Practices - United States, 2024-25 influenza season. MMWR Recomm Rep 2024;73(RR-5):1–25. doi: 10.15585/mmwr.rr7305a1
-
Immunize.org. Influenza vaccine products for the 2025–2026 influenza season. Immunize.org; 2025. Accessed August 20, 2025. https://www.immunize.org/wp-content/uploads/catg.d/p4072.pdf
-
Kharbanda EO, Vazquez-Benitez G, Romitti PA, Naleway AL, Cheetham TC, Lipkind HS, et al. First trimester influenza vaccination and risks for major structural birth defects in offspring. Vaccine Safety Datalink. J Pediatr 2017;187:234–9.e4. doi: 10.1016/j.jpeds.2017.04.039
-
Leddy MA, Anderson BL, Power ML, Gall S, Gonik B, Schulkin J. Changes in and current status of obstetrician-gynecologists' knowledge, attitudes, and practice regarding immunization. Obstet Gynecol Surv 2009;64:823–9. doi: 10.1097/OGX.0b013e3181c4bbb7
-
Mackin DW, Walker SP. The historical aspects of vaccination in pregnancy. Best Pract Res Clin Obstet Gynaecol 2021;76:13–22. doi: 10.1016/j.bpobgyn.2020.09.005
-
Nordin JD, Kharbanda EO, Vazquez Benitez G, Lipkind H, Vellozzi C, Destefano F. Maternal influenza vaccine and risks for preterm or small for gestational age birth. Vaccine Safety Datalink. J Pediatr 2014;164:1051–7.e2. doi: 10.1016/j.jpeds.2014.01.037
-
O'Leary ST, Riley LE, Lindley MC, Allison MA, Crane LA, Hurley LP, et al. Immunization practices of U.S. obstetrician/gynecologists for pregnant patients. Am J Prev Med 2018;54:205–13. doi: 10.1016/j.amepre.2017.10.016
-
Panagiotakopoulos L, McCarthy NL, Tepper NK, Kharbanda EO, Lipkind HS, Vazquez-Benitez G, et al. Evaluating the association of stillbirths after maternal vaccination in the Vaccine Safety Datalink. Obstet Gynecol 2020;136:1086–94. doi: 10.1097/AOG.0000000000004166
-
Prevention and control of influenza: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep 1997;46(RR-9):1–25.
-
Price CS, Thompson WW, Goodson B, Weintraub ES, Croen LA, Hinrichsen VL, et al. Prenatal and infant exposure to thimerosal from vaccines and immunoglobulins and risk of autism. Pediatrics 2010;126:656–64. doi: 10.1542/peds.2010-0309
-
Regan AK, Sullivan SG, Arah OA. Maternal influenza vaccination and associated risk of fetal loss: a claims-based prospective cohort study. Vaccine 2024;42:126256. doi: 10.1016/j.vaccine.2024.126256
-
Regan AK, Wesselink AK, Wang TR, Savitz DA, Yland JJ, Rothman KJ, et al. Risk of miscarriage in relation to seasonal influenza vaccination before or during pregnancy. Obstet Gynecol 2023;142:625–35. doi: 10.1097/AOG.0000000000005279
-
Sperling RS, Riley LE. Influenza vaccination, pregnancy safety, and risk of early pregnancy loss. Immunization and Emerging Infections Expert Work Group. Obstet Gynecol 2018;131:799–802. doi: 10.1097/AOG.0000000000002573
-
Stehr-Green P, Tull P, Stellfeld M, Mortenson P, Simpson D. Autism and thimerosal-containing vaccines: lack of consistent evidence for an association. Am J Prev Med 2003;25:101–6. doi: 10.1016/S0749-3797(03)00113-2
-
Thompson WW, Price C, Goodson B, Shay DK, Benson P, Hinrichsen VL, et al. Early thimerosal exposure and neuropsychological outcomes at 7 to 10 years. Vaccine Safety Datalink Team. N Engl J Med 2007;357:1281–92. doi: 10.1056/NEJMoa071434
-
Tozzi AE, Bisiacchi P, Tarantino V, De Mei B, D'Elia L, Chiarotti F, et al. Neuropsychological performance 10 years after immunization in infancy with thimerosal-containing vaccines. Pediatrics 2009;123:475–82. doi: 10.1542/peds.2008-0795
-
Verstraeten T, Davis RL, DeStefano F, Lieu TA, Rhodes PH, Black SB, et al. Safety of thimerosal-containing vaccines: a two-phased study of computerized health maintenance organization databases. Vaccine Safety Datalink Team [published erratum appears in Pediatrics 2004;113:184]. Pediatrics 2003;112:1039–48.
This information is designed as an educational resource to aid practitioners in assessing their patients’ needs, and use of this information is voluntary. This information should not be considered as inclusive of all proper treatments or methods of care or as a statement of the standard of care. It is not intended to substitute for the independent professional judgment of the treating clinician. Variations in practice may be warranted when, in the reasonable judgment of the treating clinician, such course of action is indicated by the condition of the patient, limitations of available resources, or advances in knowledge or technology. The American College of Obstetricians and Gynecologists reviews its publications regularly; however, its publications may not reflect the most recent evidence. Any updates to this document can be found on www.acog.org or by calling the ACOG Resource Center.
All ACOG committee members and authors have submitted a conflict-of-interest disclosure statement related to this published product. Any potential conflicts have been considered and managed strictly in accordance with ACOG's Conflict of Interest Disclosure Policy. The ACOG policies can be found on acog.org. The American College of Obstetricians and Gynecologists has neither solicited nor accepted any commercial involvement in the development of the content of this published product.