Number 10
This Committee Statement was developed by the American College of Obstetricians and Gynecologists' Committee on Advancing Equity in Obstetric and Gynecologic Health Care in collaboration with Adetola F. Louis-Jacques, MD, Torie Comeaux Plowden, MD, MPH, and Jamila Perritt, MD, MPH.
ABSTRACT: Disparate health outcomes and unequal access to care have long plagued many communities in the United States. Individual demographic characteristics, such as geography, income, education, and race, have been identified as critical factors when seeking to address inequitable health outcomes. To provide the best care possible, obstetrician–gynecologists should be keenly aware of the existence of and contributors to health inequities and be engaged in the work needed to eliminate racial and ethnic health inequities. Obstetrician–gynecologists should improve their understanding of the etiologies of health inequities by participating in lifelong learning to understand the roles clinician bias and personally mediated, systemic, and structural racism play in creating and perpetuating adverse health outcomes and health care experiences.
Summary of Recommendations and Conclusions
Reducing racial and ethnic inequities in health and health care should be a priority for all obstetrician–gynecologists and other health care professionals. Obstetrician–gynecologists can help meet this objective by:
-
Participating in lifelong learning to understand the roles clinician bias and personally mediated, systemic, and structural racism play in creating and perpetuating adverse health outcomes and health care experiences.
-
Adopting federal standards, at a minimum, for collection of race and ethnicity information in clinical and administrative data to analyze and identify drivers of inequities and targets for quality improvement.
-
Effectively engaging those with lived experiences of minoritization and marginalization in developing research, institutional and organizational policies, and clinical protocols and practice to advance equity.
-
Providing care with cultural humility and in a historically informed manner in efforts to build understanding, trust, and respect for patients.
-
Fostering an anti-racist culture of learning, belonging, accountability, and continued improvement for colleagues, learners, staff, and hospital administrators.
-
Acknowledging that the current system providing care for obstetric and gynecologic patients causes harm, particularly for marginalized and minoritized communities, and contributes to preventable and premature death.
-
Supporting and assisting in the recruitment, retention, and advancement of obstetrician–gynecologists and other health care professionals from racial and ethnic communities that are underrepresented in health care.
-
Promoting research that not only identifies structural and cultural barriers to care, but also prioritizes understanding these barriers and creating solutions, actively engages minoritized communities with lived experiences, and tests for the effectiveness of community-informed interventions to address racial and ethnic inequities.
-
Prioritizing policy changes that affect social and structural determinants of health and dismantle systemic racism at all levels and in all settings, such as voting rights; housing discrimination; living wages; affirmative action; and diversity, equity, and inclusion programs, with the understanding that these systems affect reproductive health outcomes for individuals and communities.
Background
Disparate health outcomes and unequal access to care have long plagued many communities in the United States. Individual demographic characteristics, such as geography, income, education, and race, have been identified as critical factors when seeking to address inequitable health outcomes. According to the United States Census Bureau, approximately 41% of U.S. females (68 million) are members of a minoritized racial or ethnic group or both 1. As of 2020, nearly one-half (49%) of U.S. births were to women of color 2, and projections suggest that, by 2050, the majority of the U.S. population will be comprised of people of color 1. As the population of the United States becomes increasingly racially and ethnically diverse, there also is a heightened awareness of the need to understand longstanding racial and ethnic inequities in reproductive health outcomes and, most importantly, an urgency to identify and address factors that contribute to these inequities (see Box 1 for a list of definitions of key terms).
Box 1.
List of Definitions
Ancestry:* A person's ethnic origin or descent, "roots," or heritage, or the place of birth of the person or the person's parents or ancestors before their arrival in the United States. Some ethnic identities, such as "German" and "Jamaican," can be traced to geographic areas outside the United States, whereas other ethnicities, such as "Pennsylvania Dutch" and "Cajun" evolved in the United States.
Anti-racism:† The active process of naming and confronting racism by changing systems, organizational structures, policies and practices, and attitudes, so that power is redistributed and shared equitably.
Bias:‡ The cognitive tendency among humans to make systematic decisions in certain circumstances based on cognitive factors rather than evidence. Bias becomes a concern when it interferes with how we make fair decisions.
Cultural Humility:§ Originally described as a tool to educate physicians to work with the increasing cultural, racial, and ethnic diversity in the United States, it is a lifelong process of self-reflection and self-critique whereby the individual not only learns about another's culture, but starts with an examination of their own beliefs and cultural identities.
Discrimination:† Treatment of an individual or group based on their actual or perceived membership in a social category, usually used to describe unjust or prejudicial treatment on the grounds of race, age, sex, gender, ability, socioeconomic class, immigration status, national origin, or religion. Discrimination by default positions some groups to have more advantages, opportunities, resources, and protections than others based on a given social characteristic or combination of social characteristics that are differentially valued.
Ethnicity:† Social construct and category based on shared geography, language, ancestry, traditions, or history. The boundaries of authenticity (ie, who or what “counts” in recognizing members of an ethnic group) often are changeable and dependent on generational, social, political, and historical situations.
Explicit Bias:|| The person is very clear about their feelings and attitudes, and related behaviors are conducted with intent. This type of bias is processed neurologically at a conscious level as declarative, semantic memory, and in words. In its extreme, it is characterized by overt negative behavior that can be expressed through physical and verbal harassment or through more subtle means such as exclusion.
Genetic Ancestry:¶ Information about the people from whom an individual is biologically descended, including their genetic relationships. Genetic information can be combined with historical information to infer where an individual's distant ancestors lived.
Health Determinants:# Areas that go beyond the social determinants and that include factors such as individual behaviors, lifestyles, and social responses to stress; biological processes, genetics, and epigenetics; the physical environment; the sociocultural environment; social determinants; and clinical events and interactions with the health care system and other systems. Each of these health determinants plays an important role in health disparities and interacts in complex ways to affect an individual's health.
Health Disparities:† Refers to a higher burden of illness, injury, disability, or mortality experienced by one group relative to another.
Health Equity:† Defined by the World Health Organization as, “the absence of avoidable, unfair, or remediable differences among groups of people, whether those groups are defined socially, economically, demographically or geographically or by other means of stratification. ‘Health equity or ‘equity in health’ implies that ideally everyone should have a fair opportunity to attain their full health potential and that no one should be disadvantaged from achieving this potential.”
Health Inequity:† Differences in health outcomes that are systematic, avoidable, unnecessary, unfair, and unjust.
Health-related Social Needs:** Social and economic needs that individuals experience that affect their ability to maintain their health and well-being. These include needs such as employment, affordable and stable housing, healthy food, personal safety, transportation, and affordable utilities.
Implicit Bias:† Unconscious mental process that stimulates negative attitudes about people outside one's own “in group” and positive attitudes or beliefs about people recognized inside one's own “in group.” Implicit racial bias leads to discrimination against people not of one's own group.
Levels of Racism:†
-
Structural or Systemic racism: The totality of ways in which societies foster racial discrimination through mutually reinforcing systems of housing, education, employment, earnings, benefits, credit, media, health care, and criminal justice. These patterns and practices in turn reinforce discriminatory beliefs, values, and distribution of resources.
-
Institutional racism: Discriminatory treatment, unfair policies and practices, and inequitable opportunities and effects within organizations and institutions, based on race. Individuals within institutions take on the power of the institution when they act in ways that advantage and disadvantage people based on race.
-
Personally mediated or interpersonal racism: The expression of racism between individuals. These are interactions occurring between individuals that often take place in the form of harassing, racial slurs, or racial jokes. It may also take more subtle forms of unequal treatment, including microaggressions.
-
Internalized racism: Acceptance by members of stigmatized races of negative messages about their own abilities and intrinsic worth.
Race:† System of categorizing people that arises to differentiate groups of people in hierarchies to advantage some and disadvantage others. Stated another way, race is a social construct or a symbolic category actively created and recreated, rather than pregiven, based on phenotype or ancestry and constructed to specific racial and historical contexts, that is misrecognized as a natural category. Although often assumed to be a biological classification, based on physical and genetic variation, racial categories do not have a scientific basis.
Racialization:† The imposition, over time, of racial differences onto a population. This process or set of processes may or may not be animated by conscious forces, rather than a static event that constructs races as real and unequal that negatively affects social, economic, and political life. It underscores the fluid and dynamic nature of race. Racialization also can be described as a form of judgmental racial classification characterizing a population group, which is used, publicly, to justify stigmatization, exploitation, and paternalism.
Racism:† As defined by Camara Jones, “racism is a system of structuring opportunity and assigning value based on phenotype (‘race’), that unfairly disadvantages some individuals and communities, unfairly advantages other individuals and communities, and saps the strength of the whole society through the waste of human resources.”
Scientific Racism:†† A historical pattern of ideologies that generates pseudoscientific racist beliefs that perpetually influence racial bias and discrimination in science and research.
Settler Colonialism:‡‡ A system or structure that perpetuates the repression of Indigenous peoples and cultures and normalizes continuous occupation by settlers; exploiting lands and resources; displacing and replacing Indigenous peoples; and erasing native lives, cultures, and histories.
Social Determinants of Health:† Refers to the underlying community-wide social, economic, and physical conditions in which people are born, grow, live, work, and age. They affect a wide range of health, functioning, and quality-of-life outcomes and risks. These determinants and their unequal distribution according to social position result in differences in health status among population groups that are avoidable and unfair.
Structural Determinants of Health:† Described by social epidemiologist Nancy Krieger as directly connected to social injustice; “political-economic systems, whereby health inequities result from the promotion of the political and economic interests of those with power and privilege (within and across countries) against the rest, and whose wealth and better health is gained at the expense of those whom they subject to adverse living and working conditions.”
*United States Census Bureau. About ancestry. Accessed June 4, 2024. https://www.census.gov/topics/population/ancestry/about.html
†American Medical Association; Association of American Medical Colleges. Advancing health equity: a guide to language, narrative and concepts. Accessed June 4, 2024. https://www.ama-assn.org/system/files/ama-aamc-equity-guide.pdf
‡National Center for Cultural Competence. Conscious and unconscious biases in health care. Establishing common ground. Accessed June 4, 2024. https://nccc.georgetown.edu/bias/module-1/1.php
§Yeager KA, Bauer-Wu S. Cultural humility: essential foundation for clinical researchers. Appl Nurs Res 2013;26:251–6. doi: 10.1016/j.apnr.2013.06.008
||National Center for Cultural Competence. Conscious and unconscious biases in health care. Establishing common ground. Accessed June 4, 2024. https://nccc.georgetown.edu/bias/module-3/1.php
¶National Human Genome Research Institute. Genetic ancestry. NHGRI; 2024. Accessed June 4, 2024. https://www.genome.gov/genetics-glossary/Genetic-Ancestry
#National Institute on Minority Health and Health Disparities. Minority health and health disparities: definitions and parameters. Accessed June 4, 2024. https://www.nimhd.nih.gov/about/strategic-plan/nih-strategic-plan-definitions-and-parameters.html
**U.S. Department of Health and Human Services. Call to action: addressing health-related social needs in communities across the nation. Accessed June 4, 2024. https://aspe.hhs.gov/sites/default/files/documents/3e2f6140d0087435cc6832bf8cf32618/hhs-call-to-action-health-related-social-needs.pdf
††National Human Genome Research Institute. Scientific racism. Accessed June 4, 2024. https://www.genome.gov/genetics-glossary/Scientific-Racism
‡‡Cox A. Settler colonialism. Accessed June 4, 2024. https://www.oxfordbibliographies.com/display/document/obo-9780190221911/obo-9780190221911-0029.xml
Although significant health inequities occur across many demographics, inequities in health outcomes and disparate access to health care services are more likely to occur among people who are marginalized and minoritized based on their racial and ethnic identities. Health conditions encountered by obstetrician–gynecologists are no exception. This is particularly true for Black and Indigenous people in the United States, who typically experience worse outcomes when compared with people in other racial and ethnic groups 3. Distinguishing between inequities in health conditions and outcomes (eg, maternal mortality) and inequities in health care services obtained (eg, receipt of mammography), as well as understanding the connection between the two, is critical.
Use of Language
ACOG recognizes and supports the gender diversity of all patients who seek obstetric and gynecologic care. In original portions of this document, authors seek to use gender-inclusive language or gender-neutral language. When describing research findings, this document uses gender terminology reported by investigators. To review ACOG's policy on inclusive language, see https://www.acog.org/clinical-information/policy-and-position-statements/statements-of-policy/2022/inclusive-language.
In addition, ACOG recognizes the heterogeneity within racialized and minoritized communities regarding their preferred descriptors. The authors particularly acknowledge variability within the Indigenous community about descriptors including, but not limited to, American Indian, Alaska Native, Native Hawaiian, Native American, First Nations, and Indigenous. In original portions of this document, authors use the term Indigenous to describe the peoples who were present in the lands and islands currently part of the United States before colonization. However, when describing or reporting research findings, this document includes the language reported by investigators. Most commonly for epidemiologic research, this will be American Indian or Alaska Native as used by the United States Census Bureau, the Centers for Disease Control and Prevention national vital records databases, and other U.S. government agency data. The authors also acknowledge that Tribal identity is a political designation rather than a race designation. However, the racialization of Indigenous peoples, and therefore structural racism, have salient effects on their health 4.
Recommendations and Conclusions
Obstetrician–gynecologists should improve their understanding of the etiologies of health inequities by participating in lifelong learning to understand the roles clinician bias and personally mediated, systemic, and structural racism play in creating and perpetuating adverse health outcomes and health care experiences. In addition, obstetrician–gynecologists and the health systems within which they operate should adopt federal standards, at a minimum, for collection of race and ethnicity information in clinical and administrative data to analyze and identify drivers of inequities and targets for quality improvement 5. Although standardization of such data facilitates analyses, federal standards currently are insufficient to accurately reflect the lived experiences of many communities. Further attention should be paid to identifying and using community-preferred or -identified language and language that differentiates ethnicity and race, that acknowledges the existence of more than one ethnicity, and that acknowledges the racialization of political and national identity among Indigenous individuals, particularly those enrolled in sovereign Tribes. Although racism creates shared exclusionary experiences among many individuals of different races, ethnicities, and nationalities that drive many health inequities, health care professionals should interrogate monolithic racial and ethnic labels to provide culturally responsive health care.
Examples of Racial and Ethnic Inequities in Obstetrics and Gynecology
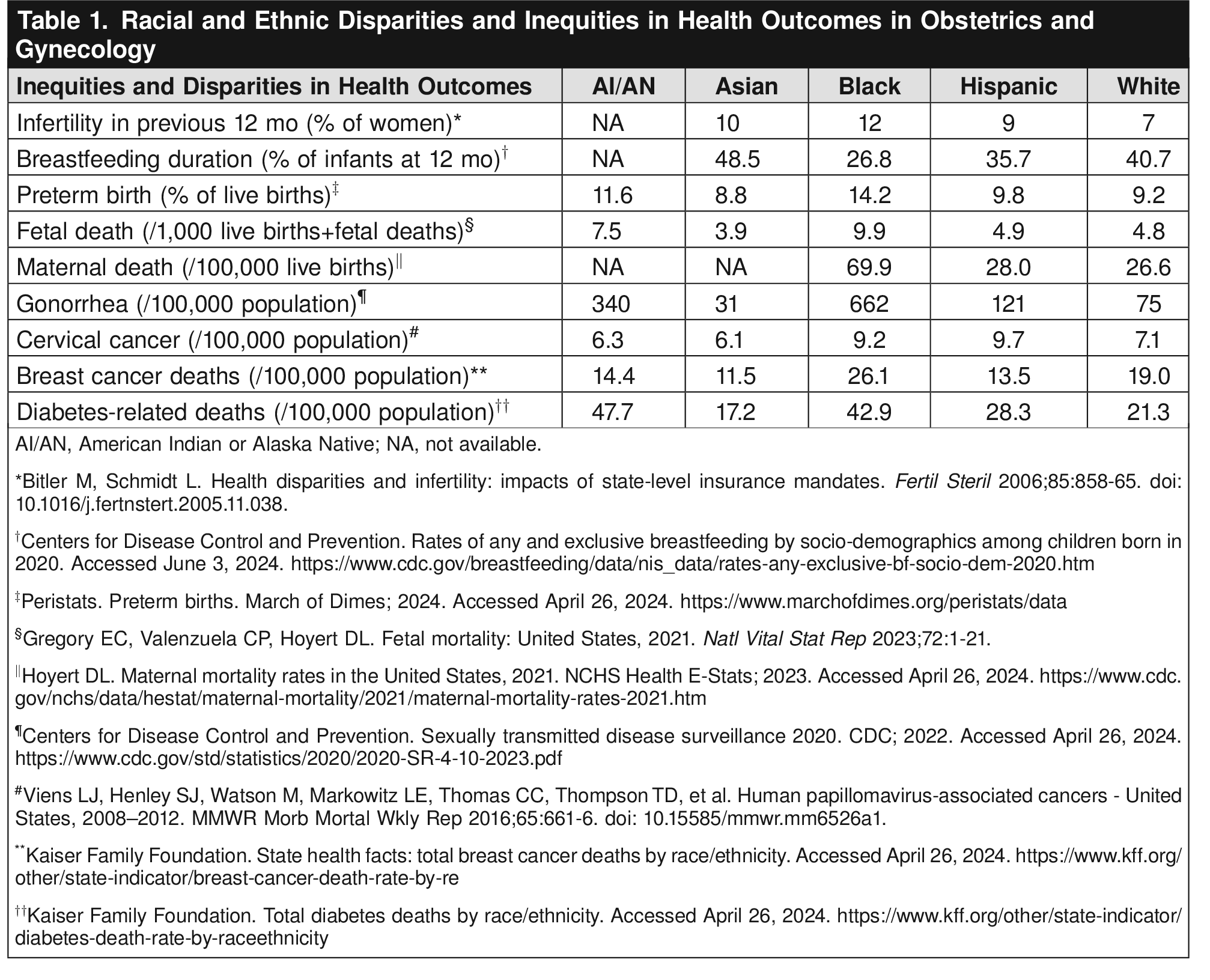
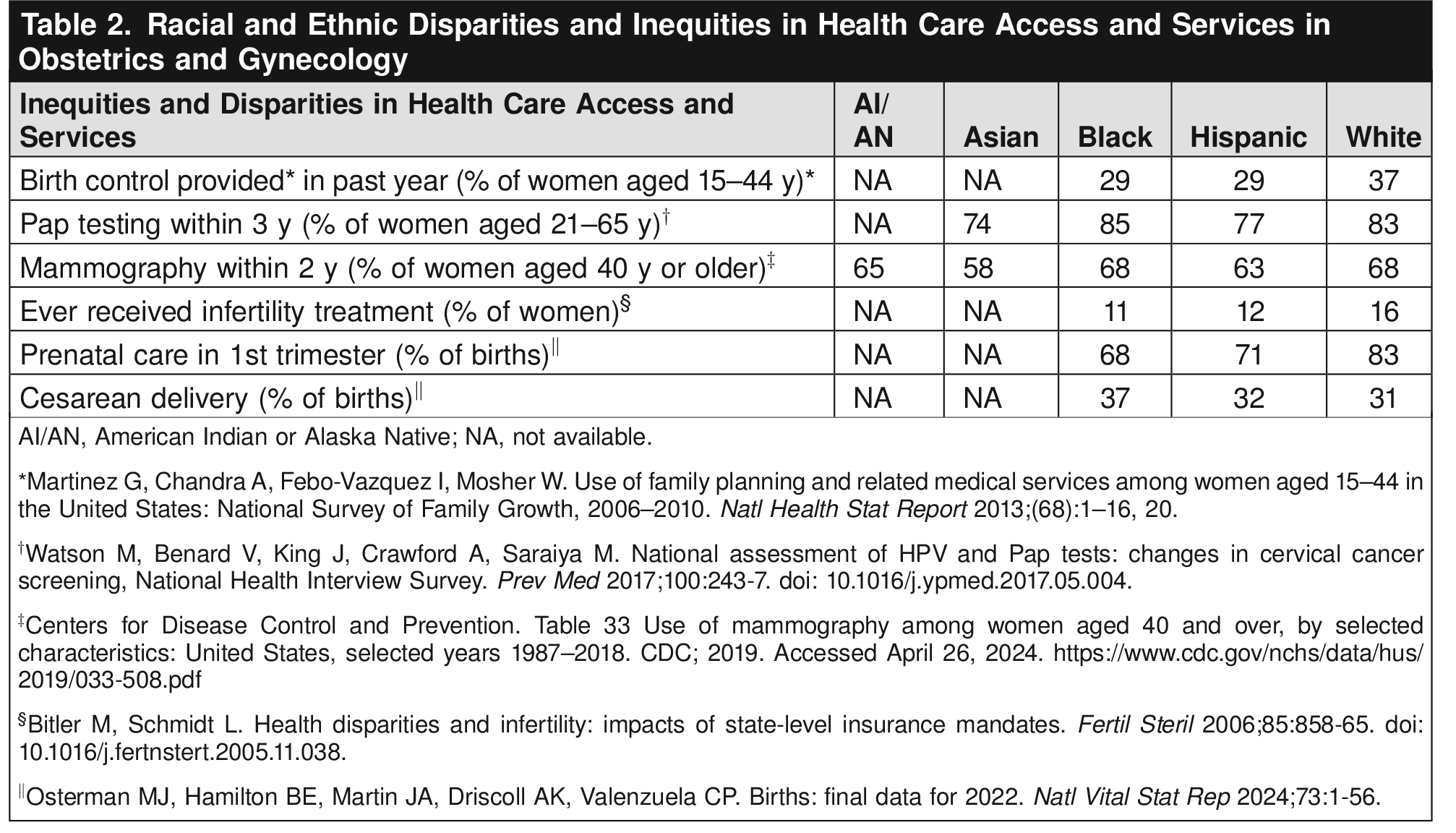
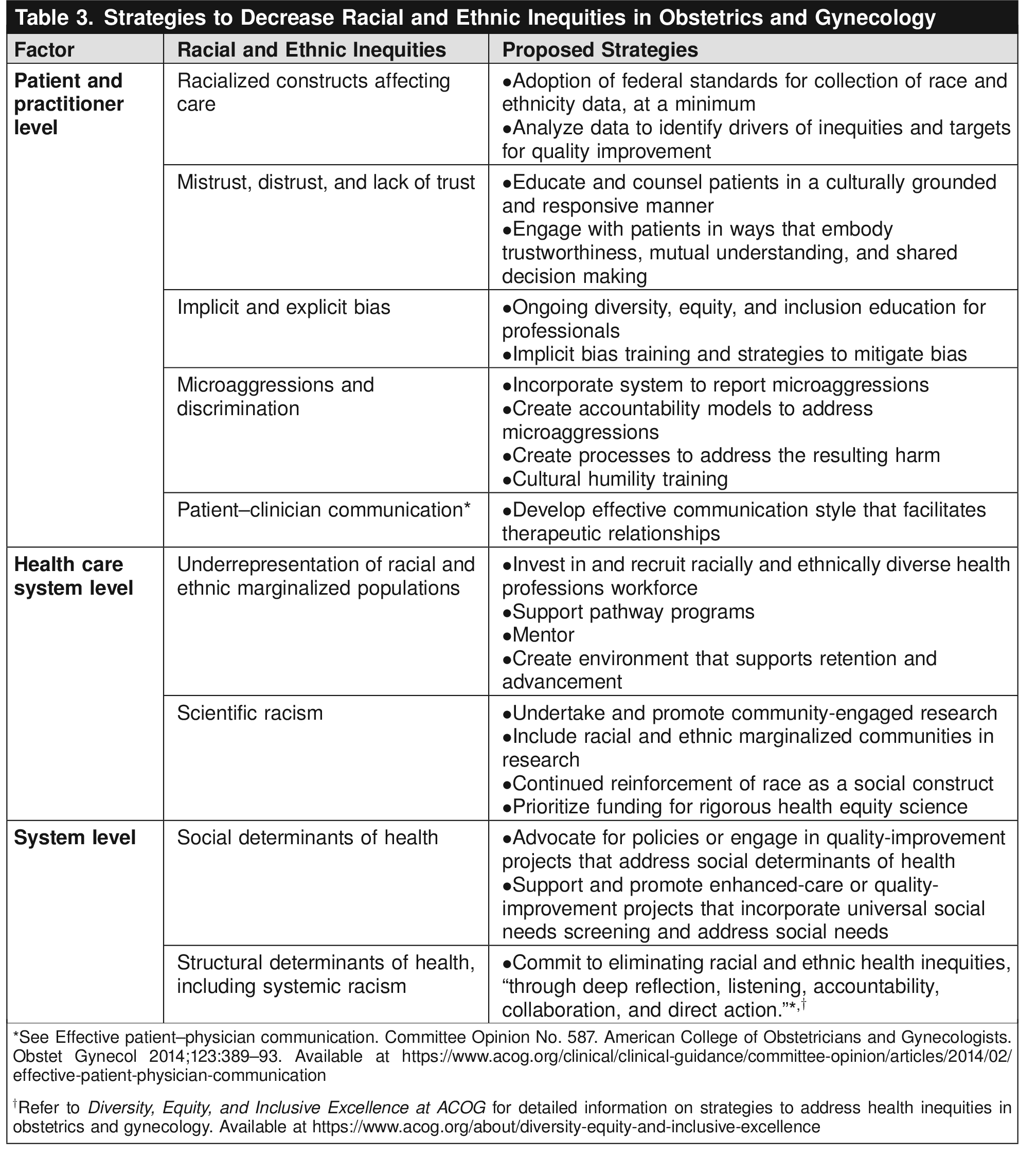
Table 1 and Table 2 present examples of key inequities in obstetrics and gynecology derived from national- or state-level data. See Table 3 for proposed solutions to racial and ethnic inequities in obstetrics and gynecology. Although the existing literature is replete with examples of differences in outcomes in Black and White individuals, more work is needed to explore inequities in health outcomes among other racial and ethnic populations, such as Indigenous, Asian, and other Pacific Islander individuals. In addition, more granular data collection on race and ethnicity would help elucidate the heterogeneity of health outcomes within the broad categories of Black, Indigenous, Hispanic, Asian, and other groups. For example, federal data collection allows for only one ethnicity, but Asian and Asian American individuals may come from more than 30 different ethnic, cultural, and national backgrounds. Similarly, Middle Eastern and Arab American individuals often are obscured within the racial category of “White.” Consolidating disparate groups into one another may conceal important inequities in outcomes. These data-aggregation issues create inequitable representation in obstetrics and gynecology outcomes studies, and lack of data in and of itself can perpetuate and uphold health inequities.



Understanding the Causes of Health Inequities
Health inequities are directly related to social and political determinants of health. Social and structural determinants of health describe environmental conditions, both physical and social, that influence health outcomes. Physical conditions such as lack of access to safe housing, clean drinking water, nutritious food, and safe neighborhoods contribute to poor health. Sociopolitical conditions such as institutional racism; police violence targeting people of color; gender inequity; discrimination against lesbian, gay, bisexual, transgender, queer+ (LGBTQ+) individuals; poverty; lack of access to quality education and jobs that pay a livable wage; and mass incarceration all shape behavior and biological processes that ultimately influence individuals' health and the health of communities. Such social conditions not only influence individual health but also work to create cycles that perpetuate intergenerational disadvantage 6. There also are factors at the patient, health care professional, health care system, and overall system levels that contribute to racial and ethnic health inequities. Analysis in the context of these differences is a part of a framework endorsed by the Institute of Medicine (now known as the National Academy of Medicine) in its 2003 report, Unequal Treatment Confronting Racial and Ethnic Disparities in Health Care 7.
Patient-Level Factors
Although race is a social construct that is not rooted in biological differences, it has real-world implications for the health and well-being of individuals 8 9. Historically, race and ethnicity have been used in medicine as markers of health risk (ie, individuals of one race may be more prone to certain diseases than those of another race). However, race and ethnicity alone do not confer disease risk 10. There is increased understanding that disparities in clinical outcomes by race are not biologically based. Instead, these racialized differences are a result of multiple factors, including the effects of systemic racism, clinician implicit or explicit bias (or both), and social and structural determinants of health. For example, the use of race and ethnicity variables in the vaginal birth after cesarean (or VBAC) calculator was discontinued because the inclusion of these variables may deter patients and clinicians from a trial of labor for Black or Hispanic individuals without biological cause, further perpetuating inequities in cesarean delivery rates, a contributing factor to maternal morbidity and mortality 11.
Epigenetics is the way that genetic expressions change as a result of an individual's behaviors or environment. Epigenetic changes can be caused by various environmental exposures and affect gene expression and, by extension, health outcomes 12. The role of how, and whether, a person manifests a disease is important to consider. For example, exposure to environmental toxins may lead to changes in the epigenome that negatively affect gametogenesis, ultimately resulting in reproductive health disorders or dysfunction 13. This is particularly critical because individuals who experience marginalization are more likely to also live in communities with higher levels of environmental toxicity and experience inequitable access to clean and healthy environments 14. Importantly, epigenetic changes also can be transmitted intergenerationally, affecting health outcomes for future generations 13.
Although individual health behaviors play a role in disease development, disease progression, and overall health, it is inaccurate, inadequate, and ineffective to attribute disparate outcomes solely to individual behaviors. To elucidate these connections, effectively engaging those with lived experiences of minoritization and marginalization in developing research, institutional and organizational policies, and clinical protocols and practice to advance equity is key. Understanding and promoting patient health is impossible without clinician engagement in understanding patients' experiences and fully considering the social, economic, and structural issues that may be contributing factors to overall health and well-being. Patient-level factors that affect health outcomes should be considered in the context of systematic factors.
Clinician-Level Factors
Although much of the research regarding the role of health care professionals in contributing to or mitigating health disparities has focused on the role of implicit bias in clinical care 15 16, both implicit and explicit bias have been shown to be important contributors to inequitable health outcomes 7. Despite the stated goal of many clinicians to deliver unbiased and impartial care, evidence indicates that health care professionals exhibit the same levels of implicit bias as seen in the wider population. Correlational evidence also indicates that biases can influence diagnosis and treatment decisions and levels of care 15. For example, racial and ethnic biases have been shown to affect clinicians' recommendations of contraceptive methods based on whom they believed to be at risk of unintended pregnancy. Data show that clinicians were more likely to recommend long-acting reversible contraceptive devices to Black and Latina women with low socioeconomic status than to White women who also presented for family planning care 17.
Moreover, studies exploring clinicians' implicit racial bias have demonstrated associations with diagnostic uncertainty, less patient-centeredness, poor professional communication, undertreatment of pain, and views of Black patients as less medically adherent than White patients, in addition to other biases that affect clinical outcomes and may contribute to health inequities 15. Some of these biases are tied to the reverberations of scientific racism and false beliefs about race-based biological differences. Many of these beliefs date back to the enslavement of Black people in the United States and were used to justify and uphold a hierarchy in the value of human life based on race (eg, the racist belief that a Black body can withstand more pain than a White body) 18, and they persist today, affecting clinical treatment courses. Research has shown that biological conceptions of race and related beliefs are associated with greater acceptance of racial disparities and even racial bias in pain perception, leading to undertreatment of pain in Black and Indigenous patients and a belief in the biological inevitability of racialized differences in health outcomes 19.
Although addressing these longstanding biases will take time and require multiple strategies, training in implicit bias is essential to begin to mitigate some of these inequities 20. Physicians and other health care professionals should understand the effects of implicit bias, work to increase self-awareness about their own biases, and display a “growth mindset”—the belief that personal characteristics can be developed 21 22 23. Obstetrician–gynecologists should provide care with cultural humility and in a historically informed manner in efforts to build understanding, trust, and respect for patients. Addressing biases can help support the creation of a safe and therapeutic environment that facilitates health equity and is inclusive of patients from various racial or ethnic backgrounds 23 24.
Just as patients can experience bias in care, learners who belong to groups that are underrepresented in medicine may also experience microaggressions (daily, commonplace, seemingly subtle behaviors and attitudes toward others that arise from conscious or unconscious bias) or outright discrimination 25 26 27 28 29. Systems to both report these issues and address the resulting harm should be readily available. Additionally, training to address bias can help all health care professionals understand and safely navigate these issues, ultimately leading to more inclusive learning environments 30 31. A diverse workforce is another strategy for achieving health equity. Inclusive and accountable learning environments are critical to stem the disproportionate attrition of Black, Indigenous, and other learners of color from the ranks of future obstetrician–gynecologists. Obstetrician–gynecologists should foster an anti-racist culture of learning, belonging, accountability, and continued improvement for colleagues, learners, staff, and hospital administrators.
Health Care System–Level Factors
Despite spending more per capita on health care expenditures than any other country 32, access to health care services in the United States is disparate and inequitable. This lack of access directly affects health outcomes, particularly for communities that have been historically marginalized from care. From access to insurance coverage, to representation in health care professions, to inclusion in scientific research, the structure and function of the health care system as it currently exists has a direct effect on health outcomes. As with the flawed health care system at large, obstetrician–gynecologists should acknowledge that the current system providing care for obstetric and gynecologic patients causes harm, particularly for marginalized and minoritized communities, and contributes to preventable and premature death.
Although the Affordable Care Act led to some improvements in insurance coverage across many demographics, people of color and those living on low incomes remain disproportionately overrepresented in those who are uninsured or underinsured. In addition, limitations on Medicaid expansion at the state level have halted improvements in access to health care. Research suggests that Medicaid expansion is linked to increased access to care and improvements in some health outcomes and has contributed to reductions in racial disparities in health coverage 33 34. Because most states that have not expanded Medicaid are in the South, where a larger proportion of residents are Black, Black adults are more likely to fall into this coverage gap 35. Additionally, undocumented immigrants are ineligible for coverage benefits under the Affordable Care Act, contributing to health inequities in these communities 36. Varying geographic availability of health care institutions, such as lengthy distances to care for many people living on Tribal reservations, also may contribute to racial and ethnic inequities in health care 37. Each of these factors should be contextualized in terms of the broader structural inequalities that permeate society, such as economic disparities, racism, gender oppression, and unequal educational opportunities 38.
Health care system–level factors, including racism, play a role in lack of representation in the medical field. The Association of American Medical Colleges defines underrepresented in medicine as races and ethnicities that are underrepresented in medicine compared with their representation in the general population; this includes Black, Mexican American, Indigenous, and mainland Puerto Rican individuals 39. According to the Association of American Medical Colleges, the number of Black men applying to and enrolling in medical school in 2014 was actually lower than it was in 1978, with 1,410 applications and 542 enrolled in 1978 compared with 1,337 applications and 515 enrolled in 2014 40. There are many barriers preventing changes in the number of people from underrepresented communities able to pursue medicine, including the belief that Black people may be less intelligent or less hardworking. The erroneous belief that standardized tests are the most important predictors of success in medical school also is partially responsible for underrepresentation of Black, Indigenous, Mexican American, and Puerto Rican students, whose scores are affected by differential learning and preparation opportunities and differential access to mentorship around the hidden curriculum (learning that occurs through, “informal interactions among students, faculty, and others,” or learning that occurs through, “organizational, structural, and cultural influences intrinsic to training institutions,” or both) 41, rather than differences in aptitude.
Furthermore, patients of color are more likely to report poor and discriminatory experiences when seeking health care, particularly when receiving care from racially discordant physicians. Specifically, Black patients reported poorer-quality communication and less information-giving during medical interactions with a physician of a discordant race 42. A large population-based study of more than 1 million hospital births in Florida found that newborn–physician racial concordance was associated with a substantial decrease in mortality of Black infants 43. Racial and ethnic concordance can improve health experiences and outcomes for Black, Indigenous, and other people of color. Furthermore, a diverse workforce in any setting is likely to improve patient–physician relationships, even when patients and physicians do not have racial concordance. These findings support continued efforts to increase the number of physicians from populations that are underrepresented in medicine and trainings on cultural humility and bias to improve interactions between physicians and patients of discordant races and ethnicities. With this in mind, obstetrician–gynecologists should support and assist in the recruitment, retention, and advancement of obstetrician–gynecologists and other health care professionals from racial and ethnic communities that are underrepresented in health care.
Scientific research and developments have contributed to increased life expectancy and improvements in public health outcomes and quality of life for many individuals. Unfortunately, these improvements are not universal. Many communities are either omitted from research studies or included as an afterthought. Moreover, the history of abuse and exploitation of many communities during the course of research, as well as deficit-based narratives that blame victims for their lack of success, may contribute to mistrust and distrust of the research process 44 45 46 47. However, literature has shown that willingness to participate in research is not associated with race or ethnicity 48. Addressing racial and ethnic underrepresentation in research in a trustworthy manner is a critical component of improving health inequities 46.
One suggested way to accomplish this in the field of clinical and translational research is by promoting research that actively involves communities with lived experiences and helps researchers understand the community's perspectives on their research priorities, barriers to care, assets, proposed solutions, and preferences for dissemination of findings 49. The community-engaged research approach provides an opportunity to amplify the voices of people and communities who have been marginalized and minoritized, to elevate and support community-informed interventions to address racial and ethnic health inequities, to support community participation in study design to facilitate culturally appropriate and accessible studies, and to explore and interrogate racialized narratives and beliefs that are held by the scientific community 46.
Finally, continued acknowledgement in research designs and scientific narratives that race has no biological basis could help mitigate scientific racism 50. Promoting research that not only identifies structural and cultural barriers to care, but also prioritizes understanding these barriers and creating solutions, actively engages minoritized communities with lived experiences, and tests for the effectiveness of community-informed interventions to address racial and ethnic inequities is a critical step in addressing and mitigating health inequities.
System-Level Factors
Social and structural determinants of health describe physical and social conditions—such as access to safe housing and nutritious food, experiencing racism and discrimination, police violence targeting people of color, lack of access to quality education, and mass incarceration—that influence various health outcomes 6. These system-level factors can have a profound effect on the health status of an individual and the health of communities.
Fundamentally, access to health opportunities is shaped by or driven by systematic oppressions such as structural racism or settler colonialism, which confine or constrain access to social and political determinants of health 51 52. For example, racial residential segregation (“redlining”) or historical confinement to Tribal reservations, two outcomes of structural racism and settler colonialism, play a significant role in defining access to social determinants of health such as wealth accumulation, political capital, education, health care resources, and economic investment.
In 2015, the American Public Health Association declared racism to be a public health crisis, and recently other professional medical societies and organizations, such as ACOG, the Centers for Disease Control and Prevention, the American Medical Association, and the Society for Maternal-Fetal Medicine, have identified racism as a public health threat and acknowledged the effects that racism has on health and well-being 53 54 55 56 57. Racism has been defined as a system that categorizes people by their physical attributes and provides advantages to some and disadvantages to others, ultimately sapping the strength of society as a whole 58. There is evidence that racism negatively affects the health of those who have experienced it 59 60 61. Women of color may be particularly vulnerable because they may face both racialized and gendered oppression, compounding the negative effects on their health 62. Obstetrician–gynecologists should prioritize policy changes that affect social and structural determinants of health and dismantle systemic racism at all levels and in all settings, such as voting rights; housing discrimination; living wages; affirmative action; and diversity, equity, and inclusion programs, with the understanding that these systems affect reproductive health outcomes for individuals and communities. Clinicians should be aware of these issues and actively engage in promoting policy changes to address racism and sexism.
Conclusion
Racial and ethnic inequities in obstetric and gynecologic outcomes and care are prevalent and persistent, and they constitute a public health crisis. To provide the best care possible, obstetrician–gynecologists should be keenly aware of the existence of and contributors to health inequities and be engaged in the work needed to eliminate racial and ethnic health inequities.
Conflict of Interest Statement
All ACOG committee members and authors have submitted a conflict of interest disclosure statement related to this published product. Any potential conflicts have been considered and managed in accordance with ACOG'’s Conflict of Interest Disclosure Policy. The ACOG policies can be found on acog.org. For products jointly developed with other organizations, conflict of interest disclosures by representatives of the other organizations are addressed by those organizations. The American College of Obstetricians and Gynecologists has neither solicited nor accepted any commercial involvement in the development of the content of this published product.