Number 8
Committee on Clinical Consensus—Obstetrics. This Committee Opinion was developed by the American College of Obstetricians and Gynecologists Committee on Clinical Consensus—Obstetrics in collaboration with committee members Alex Peahl, MD, MSc, Julia C. Phillippi, PhD, CNM, FACNM, FAAN, and Mark A. Turrentine, MD. This document has been endorsed by the following organizations: the American College of Nurse-Midwives; the Association of Physician Associates in Obstetrics and Gynecology; the Association of Women's Health, Obstetrics and Neonatal Nurses; the National Association of Nurse Practitioners in Women's Health; and the Society for Maternal-Fetal Medicine.
Summary: Prenatal care is one of the most common preventive services in the United States; it is designed to improve the health and well-being of pregnant and birthing individuals and their children through evidence-based services. Despite the prevalence of prenatal care, formalized models of prenatal care delivery have changed little since they were first published in 1930. The purpose of this Clinical Consensus document is to offer guidance on a transformative approach to the provision of prenatal care in three key areas: 1) addressing unmet social needs, 2) frequency of prenatal visits and monitoring, and 3) incorporation of telemedicine and alternative care modalities. Implementing a sustainable paradigm shift in a century-old care-delivery approach will take time; however, this document will guide maternity care professionals and their teams in the use of new prenatal care delivery models.
Background
Purpose
The purpose of this Clinical Consensus document is to offer guidance on a transformative approach to the provision of prenatal (ie, antenatal) care. Prenatal care is one of the most common preventive services in the United States 1. It is designed to improve the health and well-being of pregnant and birthing individuals and their children through evidence-based services 1, including screening, medical care, anticipatory guidance, and support (Appendix 1, available online at http://links.lww.com/AOG/E48) 1. Despite evidence-based changes in the antenatal services provided over time, the format for delivery of these services has remained largely unchanged. Prenatal care can improve the detection and management of chronic conditions and pregnancy complications, particularly for individuals with an increased risk of adverse outcomes 1 2 3 4 5.
Given the critical importance of social and structural factors associated with health and novel, evidence-based assessments and interventions in pregnancy, a change in the approach to and delivery of antenatal care is warranted. Although acknowledging the significant paradigm shift in approach to care, a change in the delivery of antenatal care is not warranted for all patients or all clinical situations. Moreover, resources to support the successful implementation of this approach are required at multiple levels, including the health care system, individual institutions, clinicians, patients, and communities.
Formalized models of prenatal care delivery have changed little since they were first published in 1930 7, with in-person visits every 4 weeks until the 7th month, every 2 weeks until the 8th month, and weekly thereafter 1 8 9 10. In response, the American College of Obstetricians and Gynecologists (ACOG) and the University of Michigan convened an independent panel of experts to provide recommendations for prenatal care delivery. The PATH (Plan for Appropriate Tailored Healthcare in Pregnancy) panel used the RAND/UCLA Appropriateness Method to develop consensus recommendations on prenatal care 12. In light of these recommendations and the current literature on prenatal care–delivery modalities 13 14 15, this document provides a guide for the provision of tailored prenatal care delivery in practice. A sustainable paradigm shift in a century-old care-delivery approach is no easy task, and implementation will not be immediate. However, the authors provide “Implementation Considerations” throughout this document to guide maternity care professionals and their teams in real-world use of new prenatal care delivery models. Additional implementation resources and information can be found on ACOG's Tailored Prenatal Care website
(https://www.acog.org/TailoredPrenatalCare).
Obstetrician–gynecologists and other maternity care professionals should refer to existing ACOG documents for guidance on recommended services to be delivered in prenatal care.
Epidemiology
In the United States, more than 3.67 million individuals give birth each year 16, and thousands experience pregnancy loss and stillbirth 17 18. Although more than 97.8% of these individuals access prenatal care, 23% do not establish care until after the first trimester of pregnancy 16 and almost half do not receive all recommended services in a timely manner 19. Social and structural drivers of health are major contributors to maternal and neonatal outcomes, both directly and indirectly, through limiting access to critical evidence-based services 20 22.
Health Equity
Birthing individuals in the United States marginalized by racism, socioeconomic status, and geography are less likely to access timely prenatal care 16 and more likely to report discrimination and bias 23 24 25, mistreatment, and a poor care experience 26 27 28. These upstream drivers are associated with important inequities in pregnancy outcomes, including maternal morbidity and mortality 31. Prenatal care tailored to the needs and preferences of each individual has the potential to improve maternal satisfaction and outcomes and improve health system functioning, especially if implemented with attention to equity 32 33 34 35 36 37 38.
Methods
This Clinical Consensus document was developed using an a priori protocol in conjunction with the authors listed above. The a priori protocol was modeled after the Clinical Consensus methodology; a full description of the Clinical Consensus methodology is published separately 39. The description below is specific to this Clinical Consensus document.
Literature Search
The Agency for Healthcare Research and Quality's (AHRQ) “Schedule of Visits and Televisits for Routine Antenatal Care” systematic review served as an evidence base for this Clinical Consensus document 14 15 32. To update the literature from the AHRQ review, the literature search conducted was limited to the end date of the AHRQ search until April 14, 2023. ACOG medical librarians searched Ovid MEDLINE and PubMed for human-only studies written in English. The search strategy from the AHRQ systematic review was used, with a few key differences: text terms were limited to those in the title or abstract, and question 3 was submitted as a separate search using the same general search, combining those results with terms for patient preference, barriers, appropriateness, and other keywords. MeSH terms and keywords can be found in Appendix 2 (available online at http://links.lww.com/AOG/E49). Search terms for racial and ethnic disparities in maternal and fetal outcomes for prenatal care were incorporated into the literature review, and recommendations were drafted with the intent to promote health equity and reduce these disparities. Bridge literature searches were completed in June 2024 and December 2024. Any updated literature was incorporated into the text and recommendations, as appropriate. When referring to specific studies found in the AHRQ systematic review, this document may cite or refer to documents published outside of the search date parameter for this literature search.
Study Selection
Qualifying studies passed both title and abstract screen and full-text screen and met the following inclusion criteria: conducted in countries ranked very high on the United Nations Human Development Index 4, included female participants, and included all study designs. Studies that passed full-text screen by the authors were included in a summary evidence map (Appendix 3, available online at http://links.lww.com/AOG/E50).
Consensus Voting and Recommendation Development
At a meeting of the Committee on Clinical Consensus—Obstetrics, a quorum of two-thirds of eligible voting members was met, and the committee held a formal vote for each proposed recommendation. All recommendation statements met or exceeded the 75% approval threshold required for consensus.
Summary of Consensus Recommendations
Obstetrician–gynecologists and other maternity care professionals should conduct a comprehensive prenatal needs assessment, including medical, social, and structural drivers of health, ideally before 10 weeks of gestation or when a pregnant individual first presents for care.
Obstetrician–gynecologists and other maternity care professionals should engage pregnant individuals in developing their care plans using shared decision making.
Obstetrician–gynecologists and other maternity care professionals should refer or coordinate assistance through the health system and community for individuals with unmet social needs.
Obstetrician–gynecologists and other maternity care professionals may adjust prenatal care delivery to be more accessible for pregnant individuals, especially for those with unmet needs.
Obstetrician–gynecologists and other maternity care professionals may tailor the visit frequency and monitoring schedule as determined by the medical and social needs of the pregnant individual.
Obstetrician–gynecologists and other maternity care professionals may offer telemedicine or other visit modalities as long as they support the completion of guideline-based recommended services.
Obstetrician–gynecologists and other maternity care professionals may individualize monitoring options for most routine parameters during pregnancy.
Consensus Recommendations and Discussion
Determining Options for Care Tailoring
Obstetrician–gynecologists and other maternity care professionals should conduct a comprehensive prenatal needs assessment, including medical, social, and structural drivers of health, ideally before 10 weeks of gestation or when a pregnant individual first presents for care.
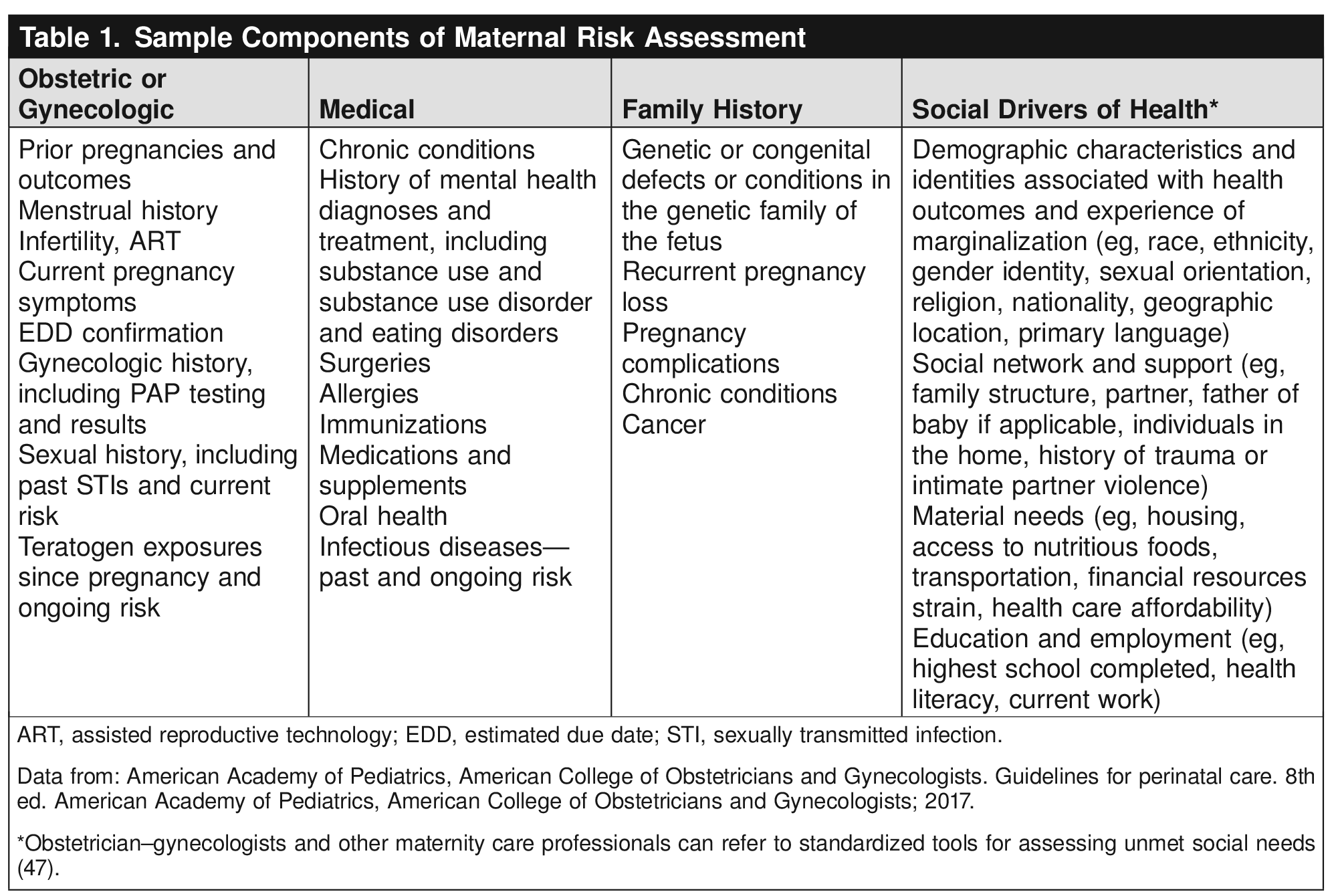
Many medical, social, and structural factors are correlated with perinatal health. An early risk assessment for all patients in pregnancy can facilitate opportunities to mitigate the adverse effects of these risk factors and to share important information and anticipatory guidance. The timing of the visit may depend on when the individual presents for care. Ideally, this assessment should be done before fertilization; if not, it should be done within a timeframe to support detection of ectopic pregnancy and modification of maternal medications and exposures during embryogenesis 12 40 41 42 43. If the pregnancy does not continue, this information can support the optimization of general health or preparation for future pregnancies.
There is limited research on the optimal timing to initiate prenatal care 13. It is reasonable to offer an initial prenatal assessment before 10 weeks from the last menstrual period or within a reasonable timeframe after discovery of pregnancy 12. More rapid assessment and evaluation by an obstetrician–gynecologist or maternity care professional may be appropriate for individuals who have medical or mental health conditions, poorly controlled pregnancy symptoms, unmet social needs, or risk factors for ectopic pregnancy 42 or who desire abortion care 44.
Implementation Considerations
Initial assessments may be completed in person or through telemedicine, depending on clinic processes and patient preference 12. Assessments and screening may be completed by any trained clinical staff (eg, medical assistants, Community Health Workers, nurses) who have received proper training in assessing medical, mental health, and social needs under the supervision of a maternity care professional 12. Physical examination components should be completed as indicated based on gestational age and individual risk factors (Appendix 1, http://links.lww.com/AOG/E48).
The assessment should include a detailed medical and reproductive history and a discussion of social and structural factors that may affect an individual's well-being and reproductive outcomes directly and through limiting access to care 1 12 45. See Table 1 for a list of potential factors to be assessed. A team-based and system-wide approach is important for overcoming social and structural issues 47. The Social Interventions Research and Evaluation Network (SIREN) also has useful implementation information 49 (see below). Maternity care professionals should reassess risk regularly and escalate care when needed 50. Sufficient time (eg, longer prenatal visits) and staff support (eg, planned contacts with nurses to complete additional risk assessments) may be considered to facilitate these extra tasks.

Additional implementation resources and information can be found on ACOG's Tailored Prenatal Care website
(https://www.acog.org/TailoredPrenatalCare).
Obstetrician–gynecologists and other maternity care professionals should engage pregnant individuals in developing their care plans using shared decision making.
Pregnancy and birth are major life events. Individuals' preferences for prenatal care delivery may be shaped by their prior health care experiences, cultural norms, and social drivers of health, such as employment, transportation, and caregiving responsibilities. Tailoring prenatal care may optimize individuals' access to services 51, care experience 12, and, ultimately, health outcomes 45 while improving operational efficiency for health systems 45.
Tailoring prenatal care requires the incorporation of patient preferences and needs for services throughout pregnancy using shared decision making. This includes discussion about the risks and benefits of preference-sensitive care options in light of the individual’s values and priorities 49. This process supports patient knowledge and autonomy, improving outcomes and satisfaction 49. See Appendix 1 http://links.lww.com/AOG/E48 for potential considerations for care tailoring.
Implementation Considerations
As pregnancy progresses, the plan of care can be adjusted based on current medical needs and patient preferences. Evidence is lacking for how best to engage patients in shared decision making, including the timing of care-planning conversations, the preferred clinician to lead conversations, and optimal supporting tools. Maternity care professionals may take into account the use of decision aids to support care-planning decisions. Practices can extend new and return prenatal visits to allow sufficient time to support effective education and shared decision making over the course of pregnancy.
Additional implementation resources and information can be found on ACOG's Tailored Prenatal Care website
(https://www.acog.org/TailoredPrenatalCare).
Tailored Care Options
a. Social Needs
Obstetrician–gynecologists and other maternity care professionals should refer or coordinate assistance through the health system and community for individuals with unmet social needs.
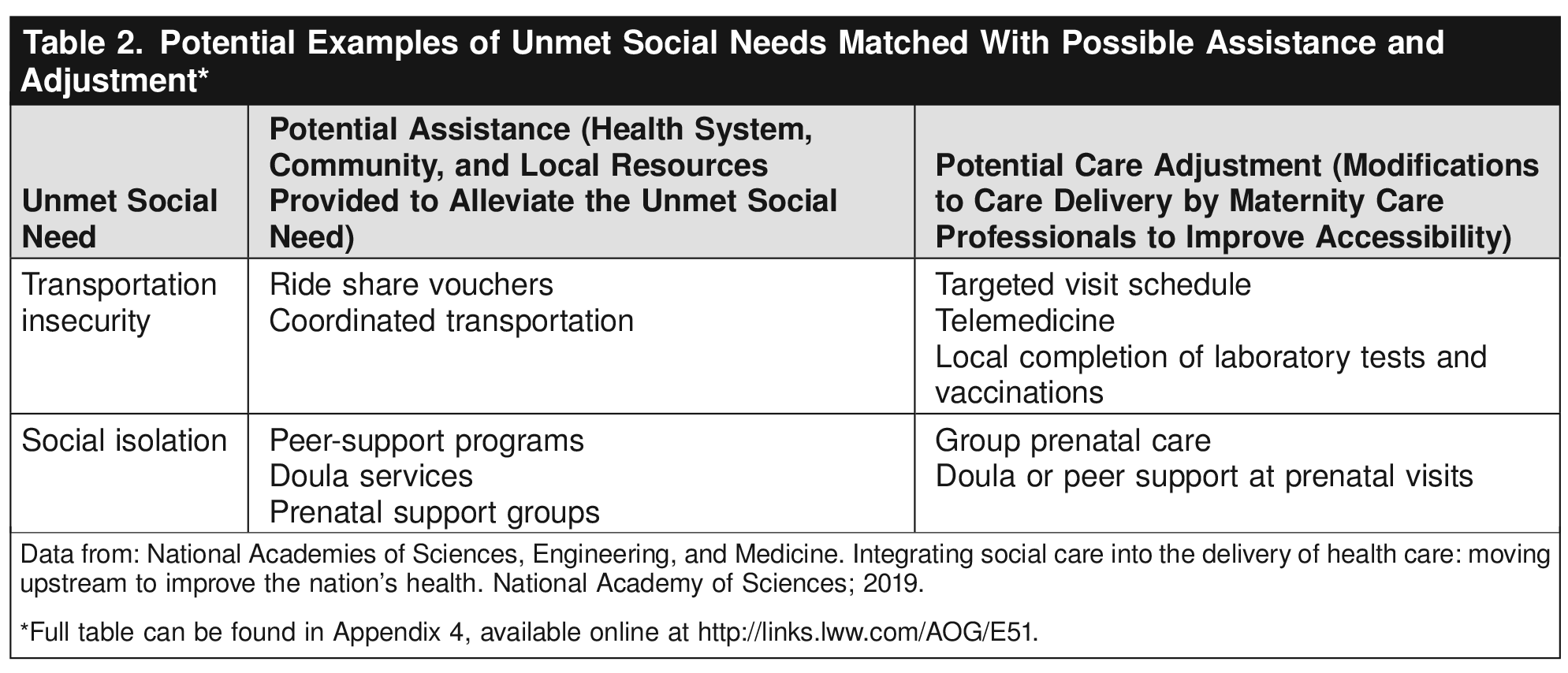
Social and structural drivers of health (eg, social isolation and food, housing, and transportation insecurity) greatly affect health outcomes, especially in the perinatal period. More information on social and structural drivers of health can be found in ACOG Committee Statement Number 11 47. See Table 2 for examples of some common unmet social needs. Assistance—provision of resources to alleviate an unmet social need—can improve the individual's access to care, reduce the negative effects of the unmet social need on maternal and neonatal outcomes, and support a more positive prenatal care experience 12 20. Assistance may take many forms and often will be specific to the need identified. Referral to other professionals (eg, social workers), where available, can provide a central point for care coordination. When these care team members are not available, regional partnerships, resource lists, and national resources such as 2-1-1 or subscriptions to social needs–prescribing programs may be used.

Though maternity care professionals may not manage social needs directly, they should remain aware of the status of unmet social needs 12. Supportive policy solutions, including public infrastructure and payment for care coordination, are needed 12.
Closed-loop processes (bidirectional communication between social service practitioners and clinicians) may achieve greater success in resolving unmet social needs when compared with providing resource lists alone 53 20. Adjustment may be used to temporarily meet needs (eg, a patient with transportation barriers awaiting ride vouchers), address ongoing social needs (eg, an hourly employee cannot afford to forgo wages), or provide adjustment in light of patient preferences for care delivery. Although there are few studies of care adjustment, models of care that address unmet social needs (eg, group prenatal care) have improved both health and patient-reported outcomes 55 56. The National Academy of Medicine supports this approach as part of an overall strategy to address unmet social needs 20.
Maternity care professionals should recognize the social and structural drivers of health that affect patients' ability to make or maintain prenatal appointments and be prepared to offer care adjustments. Potential care adjustments include 1) tailored visit schedules (vs traditional) streamlined around needed education and services; 2) telemedicine (vs in-person care) where possible to reduce travel burden, need for childcare, or time away from work 32 57 58; and 3) group prenatal care (vs individual care, ideally in the individual's native language) to address social isolation and low health literacy 55. Adjustments should incorporate the individual's medical and social risk factors and ensure the timely provision of evidence-based services 12.
Implementation Considerations
Although assistance often requires input from health system and community resources, many adjustments can be completed by the maternity care professional even if additional resources are not available when changes to routine practices are initially made. For assistance, partnering with local and regional organizations, such as Perinatal Quality Collaboratives, local ACOG Districts and Sections, and community-based organizations to generate and maintain lists of available resources, can help maternity care professionals map social and structural drivers of health and available resources in their health system and community. Adjustments will depend on the local care context and availability of alternative prenatal care–delivery models (eg, telemedicine, group care).
For patients with unmet social needs, additional prenatal visits with a maternity care professional are unlikely to address underlying needs and may create additional burden 12. Potential options for assistance and adjustment are listed in Table 2 to demonstrate linkages and approaches that may be available to alleviate unmet social needs; however, these specific resources may not be available in all communities or health systems. Increased demands on physicians and other health care professionals to address unmet social needs with insufficient resources have been associated with burnout 59. Reimbursement, resources, and workforce development may be able to support frontline workers in expanding social services into medical care. Care adjustment may also help reduce burnout by giving maternity care professionals an immediate tool to address unmet social needs.
Additional implementation resources and information can be found on ACOG's Tailored Prenatal Care website
(https://www.acog.org/TailoredPrenatalCare).
b. Frequency
Obstetrician–gynecologists and other maternity care professionals may tailor the visit frequency and monitoring schedule as determined by the medical and social needs of the pregnant individual.
Prenatal care traditionally has been delivered using a visit schedule of 12–14 in-person visits, regardless of individual risk factors 1. Three systematic reviews have demonstrated equivalent maternal and neonatal outcomes and an overall positive care experience with targeted visit schedules using 6–10 visits for average-risk individuals without medical or pregnancy complications 13 15 60. Tailored visit schedules that adjust the number and frequency of prenatal visits based on risk and parity have been supported by several organizations and peer nations for more than two decades 13 15 60 63.
Though routine measurement of key parameters, including maternal blood pressure, weight, fundal height, and fetal heart tones, are traditional in prenatal care 1, little is known about the optimal frequency of these measures 13 3 64 65. In the absence of evidence, it is reasonable to continue routine measurement of these parameters at the same frequency as routine prenatal care visits for individuals not at increased risk of complications 66. No routine antenatal measurement of fetal well-being (eg, measuring fetal heart rate, formal kick counts) has demonstrated benefit for stillbirth prevention 67 68. Outside of select maternal or fetal conditions (eg, metabolic disorders or cardiac conditions,) or specific indications for antenatal testing (eg, maternal chronic hypertension, fetal growth restriction), there is no additional utility in checking fetal heart rate if the patient can confirm fetal movement 13 3 66 69 70. There may be nonclinical benefits to checking fetal heart tones, including reduction in maternal anxiety, improved parental bonding with the neonate, and an improved patient experience 63 71. Individuals with chronic hypertension or hypertensive disorders of pregnancy may benefit from more-frequent blood pressure measurements 66. See below for discussion of the modality of monitoring, including self-monitoring.
Assessment of fetal growth is important for the detection of fetal growth restriction, macrosomia, and potential sequelae 1. Fundal height is the primary screening tool for assessing fetal growth and should be completed with routine in-person visits after 24 weeks of gestation 72. If fundal height measurement is not feasible or there are other indications for serial ultrasonographic assessment of growth, ultrasonograms may replace routine fundal height measurement 72. There is limited evidence on the utility of other screening measures (eg, universal third-trimester growth ultrasonogram) compared with fundal height assessment in individuals without risk-factors for poor fetal growth 72.
Measurement of maternal weight gain can be used to diagnose hyperemesis and assess risk for adverse perinatal outcomes, such as gestational diabetes, hypertensive disorders, and risk of cesarean birth 73. Routine measurement alone of maternal weight has not been associated with reductions in gestational weight gain or development of diabetes 13. However, behavioral interventions to prevent excessive weight gain have been shown to have improvements in maternal and birth outcomes. Maternity care professionals can work actively to mitigate stigma against individuals with overweight or obesity, particularly when discussing nutrition and weight gain with patients 74. It is reasonable to continue routine measurement of these parameters at the same frequency as routine prenatal care visits for individuals not at risk of complications 66. Adjustments in weight-gain assessment, such as not displaying the numeric weight to the patient, can be made for patients with a history of eating disorders 75.
Routine dipstick measurement of urine protein is no longer recommended as part of standard prenatal care assessments, given its low diagnostic accuracy 76 77.
Implementation Considerations
Tailored visit schedules may provide advantages for individual patients, such as reduced travel, time accessing care, and associated costs while supporting the completion of evidence-based services 63 78. For health systems, adjusting the number of appointments for average-risk individuals can improve availability for patients with more complex needs 66. Still, tailored care does not mean less care; patient assessments, including medical and social risk factors, as well as visit planning, require more time than with prior prenatal care models. Further, health systems can consider increasing visit length for patients receiving tailored visit schedules to maintain the overall time patients spend with their maternity care professional, even though the overall number of visits may be decreased. Patients should have access to a clinician to ask questions or triage concerns between visits, particularly with longer intervals between scheduled contacts. Future work is needed to assess the effects of new care models on operational efficiency and access to care.
Additional implementation resources and information can be found on ACOG's Tailored Prenatal Care website
(https://www.acog.org/TailoredPrenatalCare).
c. Modality
Obstetrician–gynecologists and other maternity care professionals may offer telemedicine or other visit modalities as long as they support the completion of guideline-based recommended services.
Many alternative approaches to prenatal care delivery have emerged in recent decades, including telemedicine (eg, video or audio-only) and group prenatal care. Telemedicine is effective for medical care when in-person services (eg, physical examinations, laboratory tests, imaging, vaccinations) are not needed or can be completed through alternative means 66 79. Sample schedules of in-person and telemedicine visits for average-risk and greater-than-average\x{2013}risk patients based on routine recommended services are provided in Appendix 1 http://links.lww.com/AOG/E48. These visit schedules should be tailored as part of developing a patient-centered care plan. Greater-than-average–risk individuals may require greater intensity of follow-up and potential referral for subspecialist care, including maternal–fetal medicine care, which isn't covered by this sample schedule.
Telemedicine can improve access to services, reduce patient and health system costs 80 81 82 83 84, and improve patient experience 31 37 84 85 86. If access to care is increased through telemedicine visits, perinatal outcomes are equivalent to or improved when compared with in-person visits 84 86 87 88 89 90 91. In observational studies, not all patients preferred telemedicine care compared with in-person visits 92 93 94 95. Satisfaction gains may be greatest for those who live the farthest from their care location 96. A 2023 systematic review including two randomized controlled trials, four nonrandomized comparative studies, and one survey reported equivalence of maternal and neonatal outcomes and improved maternal experience of care with telemedicine. However, the models of care were heterogeneous (one to six visits), the quality of evidence was low, and studies were underpowered to detect rare outcomes 14. The research on effects of telehealth on maternal mental health is mixed and may be confounded by prior maternal conditions, anxiety related to the COVID-19 pandemic, and heterogeneity in mental health interventions 14 15 32 97 98. Observational studies demonstrate that telehealth may be especially beneficial for interprofessional care or consultations 32 99 100.
Another prenatal care modality, group prenatal care, incorporates additional education and peer support through group visits. Individual studies have demonstrated improved clinical and patient-reported outcomes of group care compared with individual care, including preterm birth, neonatal intensive care unit admission, patient satisfaction with care, knowledge of pregnancy topics, and breastfeeding initiation and continuation 55. A meta-analysis including 10 observational studies and four randomized controlled trials did not demonstrate improvements in maternal or neonatal outcomes overall, though subgroup analysis did show a reduction in preterm birth for African American patients with low incomes (relative risk 0.55; 95% CI, 0.34–0.88) 55 101. Marginalized individuals who experience care inequities, stigma, and bias, including those from minoritized racial and ethnic groups, those living with human immunodeficiency virus (HIV), and adolescents, may experience more benefit from this model, especially if groups are organized around a shared identity or condition 55.
Implementation Considerations
Ambulatory practice preparation for the implementation of telehealth, including attention to workflow, educational content of visits, and adequate allotment of time for the visit, may improve the experience of telehealth for patients and clinicians 57 102 103 104. It is important that patients have access to necessary equipment with audio or video if planning telemedicine care; infrastructure such as broadband internet or reliable cell service with adequate bandwidth is also needed for successful communication 58 63 66 105. There is no evidence that video visits are superior to audio-only encounters. Video visits may support rapport-building, communication, and insight into the patient's home setting, or they may be seen by patients as surveillance and an invasion of privacy 63 95. Health care professionals interested in telemedicine or group prenatal care may reference ACOG Committee Opinion Number 798, Implementing Telehealth in Practice, and ACOG Committee Opinion Number 731, Group Prenatal Care 55 79.
Additional implementation resources and information can be found on ACOG's Tailored Prenatal Care website
(https://www.acog.org/TailoredPrenatalCare).
Obstetrician–gynecologists and other maternity care professionals may individualize monitoring options for most routine parameters during pregnancy.
Monitoring of routine parameters in pregnancy is increasingly available outside of clinical settings, such as at local pharmacies, through home-visiting programs, or by remote self-monitoring. Evidence demonstrates the feasibility, acceptability, and accuracy of self-monitoring of blood pressure and weight 13. Fewer data are available on self-monitoring of obstetric assessments, including fetal heart tones and fundal height. The PATH panel concluded that self-monitoring of blood pressure and weight could be completed in any trimester, and self-monitoring of fetal heart tones and fundal height could be completed in the second and third trimesters if deemed appropriate by the maternity care professional 12.
Implementation Considerations
Self-measurement of routine parameters is reasonable if the patient: 1) desires self-monitoring; 2) has adequate training to complete the measurement accurately; 3) can access necessary, appropriate, reliable equipment; 4) is aware of abnormal parameters; and 5) has means to obtain help with abnormal results 31 65. Cost of home devices remains a barrier to self-monitoring for many individuals, and future policies are needed to improve equitable access 31 63 65 66 106.
Additional implementation resources and information can be found on ACOG's Tailored Prenatal Care website
(https://www.acog.org/TailoredPrenatalCare).
Future Research
Research on prenatal care delivery, including visit frequency and modality, has been limited by several factors. Bundled and global billing for prenatal care makes many visit numbers and modalities invisible in claims data sets 107. In studies in which the effectiveness of prenatal care is assessed, definitions of quality and outcomes are heterogeneous, preventing meta-analysis 32. In addition, social drivers of health are not assessed routinely, and their confounding effects cannot be disentangled 108.
Guidelines are effective only if used. Further work is needed to define the facilitators, barriers, and most effective strategies for implementing person-centered, tailored prenatal care. Implementation strategies should carefully consider how new models affect the patient experience of care. Although tailored prenatal care may improve operational efficiency and access to care, research should ensure it does not do so at the expense of patients, particularly those historically marginalized by the health system. A diverse group of participants from multiple stakeholder groups, including patients, families, community members, and health care workers, should be included in future studies to ensure broad input to address the needs of the populations being served.
Use of Language
ACOG recognizes and supports the gender diversity of all patients who seek obstetric and gynecologic care. In original portions of this document, the authors seek to use gender-inclusive language or gender-neutral language. When describing research findings, this document uses gender terminology reported by the investigators. ACOG's policy on inclusive language can be reviewed at https://www.acog.org/clinical-information/policy-and-position-statements/statements-of-policy/2022/inclusive-language.
Appendices
Supplemental Digital Content
Sample schedules for prenatal care services and visit frequency: http://links.lww.com/AOG/E48
Literature search with keywords and PICO: http://links.lww.com/AOG/E49
Evidence maps: http://links.lww.com/AOG/E50
Examples of unmet social needs with possible assistance and adjustments: http://links.lww.com/AOG/E51
Conflict of Interest Statement
All ACOG committee members and authors have submitted a conflict of interest disclosure statement related to this published product. Any potential conflicts have been considered and managed in accordance with ACOG's Conflict of Interest Disclosure Policy. The ACOG policies can be found on acog.org. For products jointly developed with other organizations, conflict of interest disclosures by representatives of the other organizations are addressed by those organizations. The American College of Obstetricians and Gynecologists has neither solicited nor accepted any commercial involvement in the development of the content of this published product.